
These authors measured synovial fluid levels of 9 cytokines (interleukin [IL] 6, granulocyte-macrophage colony-stimulating factor, IL-1β, IL-12, IL-2, IL-8, interferon-γ, IL-10, and tumor necrosis factor-α) in 75 cases of revision shoulder arthroplasty with a multiplex immunoassay. Cases were classified into infection categories and groups based on objective perioperative findings.
The culture results were as shown below

They found that synovial IL-6, granulocyte-macrophage colony-stimulating factor, interferon-γ, IL-1β, IL-2, IL-8, and IL-10 were significantly elevated in cases of revision shoulder arthroplasty classified as infected.
Individually, IL-6, IL-1β, IL-8, and IL-10 showed the best combination of sensitivity and specificity for predicting infection, and a combined cytokine model consisting of IL-6, tumor necrosis factor-α, and IL-2 showed better diagnostic test characteristics than any cytokine alone, with sensitivity of 0.80, specificity of 0.93,, positive and negative predictive values of 0.87 and 0.89, and positive and negative likelihood ratios of 12.0 and 0.21.
While there were significant differences among the groups, the graphs below show the overlap in individual cytokine levels for the control, no infection and infection groups,


and in the no growth and Propionibacterium groups.


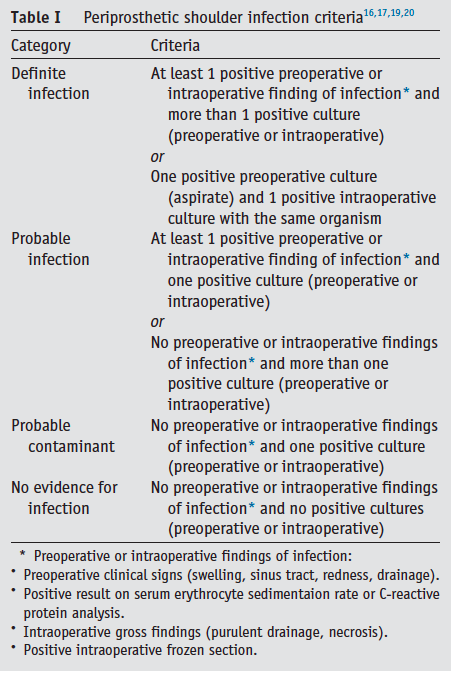
Comment: The definitions used to define a periprosthetic shoulder infection continue to vary among authors. Many schemes are complex and challenging to apply. Preoperative or intraoperative findings of infection, such as swelling, sinus tract, redness, drainage, elevated serum erythrocyte sedimentaion rate or C-reactive protein, intraoperative purulent drainage, necrosis, or positive intraoperative frozen sections constitute signs of 'obvious' infections. However, Propionibactium often manifest a 'stealth' presentation of pain, stiffness and component loosening after a 'honeymoon' of good post arthroplasty function. Inflammatory cytokines are more likely to be elevated in the 'obvious' cases than in the 'stealth' cases.
These authors have done a lot of good work on the analysis of synovial fluid in cases of revision arthroplasty. It will be of interest to see how effective cytokine analysis is in the prediction of positive cultures where the 'obvious' signs of infection are absent.
===
Use the "Search" box to the right to find other topics of interest to you.
You may be interested in some of our most visited web pages including:shoulder arthritis, total shoulder, ream and run, reverse total shoulder, CTA arthroplasty, and rotator cuff surgery as well as the 'ream and run essentials'
You may be interested in some of our most visited web pages including:shoulder arthritis, total shoulder, ream and run, reverse total shoulder, CTA arthroplasty, and rotator cuff surgery as well as the 'ream and run essentials'