
Shoulder arthroplasty is performed through a transection of the subscapularis attachment to the humerus. Regardless of the method of detachment, careful repair and postoperative protection of the repair are necessary to prevent failure of the reattachment (see this link).
Failure of the subscapularis to regain its normal function after arthroplasty is not uncommon (see The subscapularis - does it ever recover after shoulder arthropllasty - peel vs LTO?).
Evidence of subscapularis failure may be a sensation of anterior instability as suggested by this axillary view

increased range of passive external rotation

or loss of strength on the belly press test (on the left below, the patient is showing the normal ability to press the hand into the belly keeping the elbow in the plane of the body; on the right weakness of the subscapularis is indicated by the patient's extending the shoulder to generate pressure on the belly).

If a traumatic failure of the subscapularis occurs soon after the shoulder arthroplasty a primary repair may be successful.
Failure of the subscapularis to regain its normal function after arthroplasty is not uncommon (see The subscapularis - does it ever recover after shoulder arthropllasty - peel vs LTO?).
Evidence of subscapularis failure may be a sensation of anterior instability as suggested by this axillary view
increased range of passive external rotation

or loss of strength on the belly press test (on the left below, the patient is showing the normal ability to press the hand into the belly keeping the elbow in the plane of the body; on the right weakness of the subscapularis is indicated by the patient's extending the shoulder to generate pressure on the belly).

If a traumatic failure of the subscapularis occurs soon after the shoulder arthroplasty a primary repair may be successful.
If the tendon tissue is of insufficient quantity or quality, a reconstruction using allograft can be considered. In this reconstruction, it is necessary to release adhesions and mobilize the subscapularis with great care due to the close proximity of neurovascular structures and altered surgical field with scar tissue.
After the subscpularis is mobilized, a burr is used to create a transosseus tunnel in the bicipital groove separated by a 2cm bone bridge as shown below for a left shoulder.

Tendon allograft is passed through this tunnel

and then each end was woven through the native subscapularis tendon medially.

Tendon allograft is passed through this tunnel

and then each end was woven through the native subscapularis tendon medially.


After securing what remains of the native subscapularis to the lesser tuberosity with sutures, the allograft is looped over itself in a figure of 8 and secured laterally with suture. The reconstruction is set to limit external rotation to zero degrees.
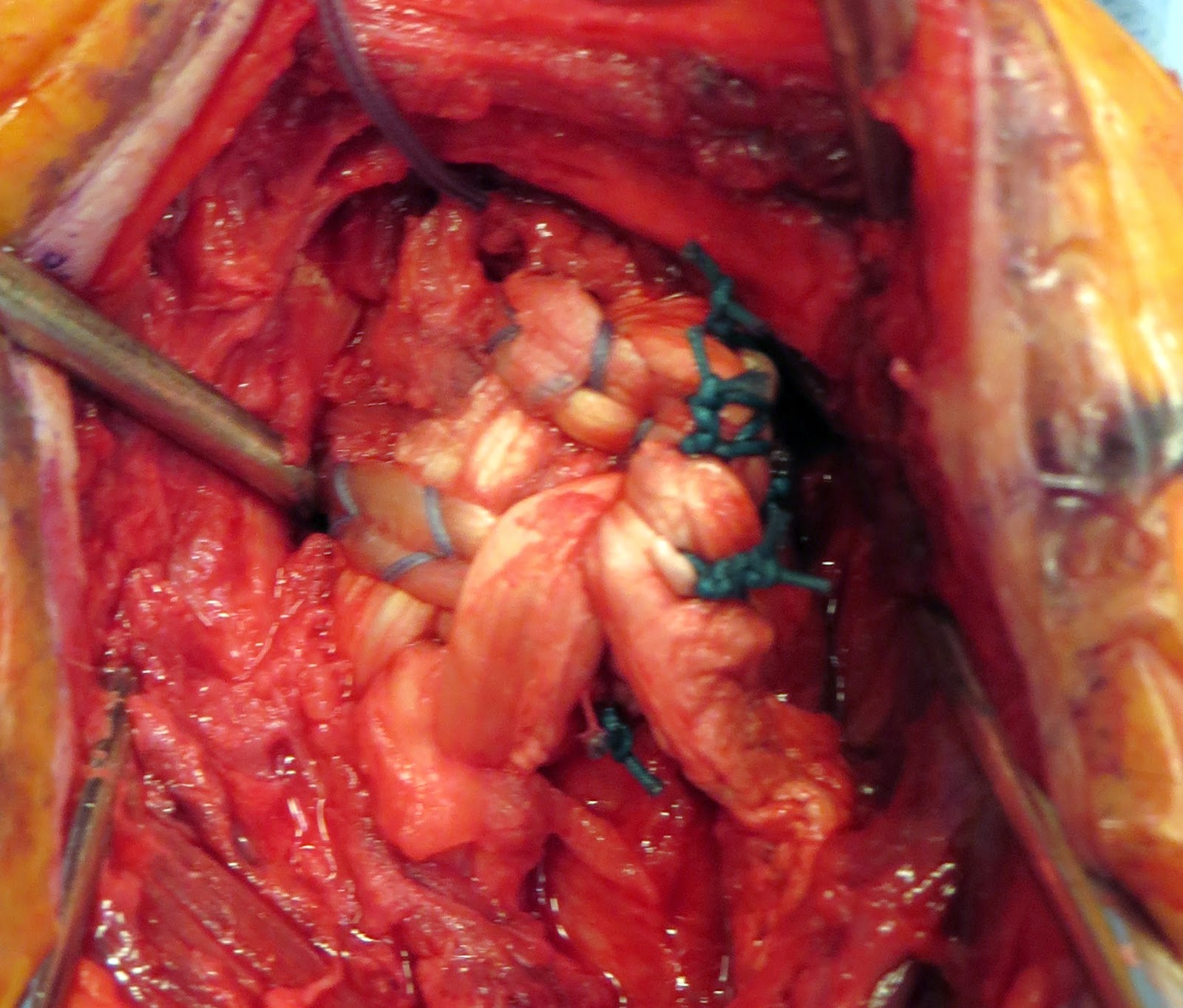

The shoulder is protected in a sling for six weeks. Passive external rotation stretching is permanently avoided.
If there is no subscapularis that can be used for an allograft reconstruction, an anterior capsular reconstruction is considered. Drill holes are placed in the anterior glenoid, as shown below for a right shoulder.



 The shoulder is protected in a sling for six weeks. Passive external rotation stretching is permanently avoided.
The shoulder is protected in a sling for six weeks. Passive external rotation stretching is permanently avoided.

Holes are also created at the base of the lesser tuberosity

Tendon graft is passed through the holes.

and tied, limiting external rotation to zero degrees. Any available subscapularis is tied into the allograft reconstruction.

===
Use the "Search" box to the right to find other topics of interest to you.
You may be interested in some of our most visited web pages including:shoulder arthritis, total shoulder, ream and run, reverse total shoulder, CTA arthroplasty, and rotator cuff surgery as well as the 'ream and run essentials'
You may be interested in some of our most visited web pages including:shoulder arthritis, total shoulder, ream and run, reverse total shoulder, CTA arthroplasty, and rotator cuff surgery as well as the 'ream and run essentials'