
In 1990, the late Doug Harryman published Translation of the humeral head on the glenoid with passive glenohumeral motion in which he described the effects of anterior capsular tightness on posterior humeral head translation in osteoarthritis. Here is a figure from that article.

The effect of anterior capsular tightness was further described in Practical Evaluation and Management of the Shoulder (see this link)


illustrating that this posterior translation can result in posterior glenoid wear
 In Edge displacement and deformation of glenoid components in response to eccentric loading. The effect of preparation of the glenoid bone, Collins et al found that the thickness of glenoid articular cartilage was greatest in its posterior aspect, making this part of the glenoid socket at greatest risk for wear. In the case of the type B1 glenoid - where there is no obvious bony biconcavity - there is in fact a biconcavity in the articular surface due to loss of this posterior glenoid articular cartilage.
In Edge displacement and deformation of glenoid components in response to eccentric loading. The effect of preparation of the glenoid bone, Collins et al found that the thickness of glenoid articular cartilage was greatest in its posterior aspect, making this part of the glenoid socket at greatest risk for wear. In the case of the type B1 glenoid - where there is no obvious bony biconcavity - there is in fact a biconcavity in the articular surface due to loss of this posterior glenoid articular cartilage.  which progresses to posterior glenoid bone wear becoming a type B2 glenoid
which progresses to posterior glenoid bone wear becoming a type B2 glenoid

as revealed by the axillary "truth" view 
This posterior decentering is associated with loss of external rotation

Thus we have the vicious circle in which tightness and stiffness of the anterior capsule leads to posterior decentering of the humeral head leading to erosion of the posterior articular cartilage and bone which leads to limited external rotation leading to more tightness and stiffness of the anterior capsule.

as illustrated here: 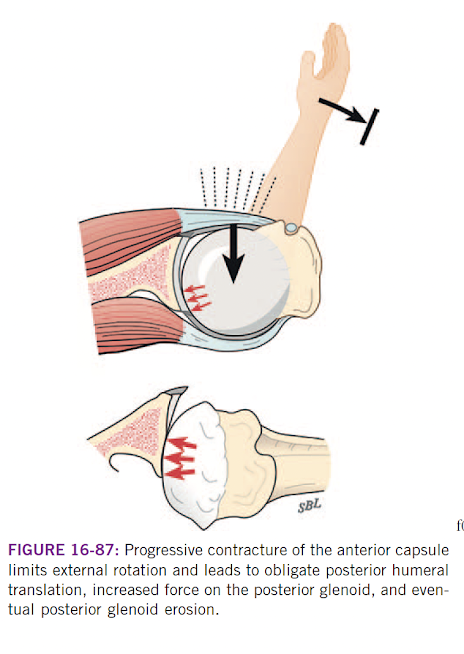 A recent article The Association Between Anterior Shoulder Joint Capsule Thickening and Glenoid Deformity in Primary Glenohumeral Osteoarthritis builds on these points. These authors sought to determine the relationship between anterior capsular thickening and glenoid deformity in primary glenohumeral osteoarthritis in 134 osteoarthritic shoulders with magnetic resonance imaging (MRI) and computed tomography (CT) scans.
A recent article The Association Between Anterior Shoulder Joint Capsule Thickening and Glenoid Deformity in Primary Glenohumeral Osteoarthritis builds on these points. These authors sought to determine the relationship between anterior capsular thickening and glenoid deformity in primary glenohumeral osteoarthritis in 134 osteoarthritic shoulders with magnetic resonance imaging (MRI) and computed tomography (CT) scans.

They found that the anterior capsule was thickest in glenoid types B2 (5.5 mm) and B3 (6.1 mm), and thinnest in A1 (3.7 mm). Adjusted for age and sex, glenoid types B2 and B3 showed the strongest association with increased anterior capsule thickness, compared to glenoid type A1. Increased capsular thickness correlated with greater glenoid retroversion and posterior humeral head subluxation. In multivariable analysis, for every 1-mm increase in anterior capsular thickening, there was an adjusted mean increase of 3.2 degrees in glenoid retroversion and a 3.8% increase in posterior humeral head subluxation.
Taken together, these observations bring up the question: can interventions (such as mobilization exercises or anterior capsular releases) implemented early in the course of osteoarthritis interrupt the vicious cycle?
You can support cutting edge shoulder research that is leading to better care for patients with shoulder problems, click on this link.
Follow on twitter: https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interestShoulder arthritis - what you need to know (see this link).How to x-ray the shoulder (see this link).The ream and run procedure (see this link).The total shoulder arthroplasty (see this link).The cuff tear arthropathy arthroplasty (see this link).The reverse total shoulder arthroplasty (see this link).The smooth and move procedure for irreparable rotator cuff tears (see this link).Shoulder rehabilitation exercises (see this link).








They found that the anterior capsule was thickest in glenoid types B2 (5.5 mm) and B3 (6.1 mm), and thinnest in A1 (3.7 mm). Adjusted for age and sex, glenoid types B2 and B3 showed the strongest association with increased anterior capsule thickness, compared to glenoid type A1. Increased capsular thickness correlated with greater glenoid retroversion and posterior humeral head subluxation. In multivariable analysis, for every 1-mm increase in anterior capsular thickening, there was an adjusted mean increase of 3.2 degrees in glenoid retroversion and a 3.8% increase in posterior humeral head subluxation.
You can support cutting edge shoulder research that is leading to better care for patients with shoulder problems, click on this link.
Follow on twitter: https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link).
Shoulder rehabilitation exercises (see this link).