
A large industry has formed around the assessment of, planing for, special components to address, and surgical "correction" of glenoid retroversion to 15 degrees or less in performing an anatomic total shoulder arthroplasty.


In Do glenoid retroversion and humeral subluxation affect outcomes following total shoulder arthroplasty? the authors studied 113 patients at an average of 4 years after arthroplasty. Retroversion and humeral head subluxation before and after surgery were measured on axillary radiographs.
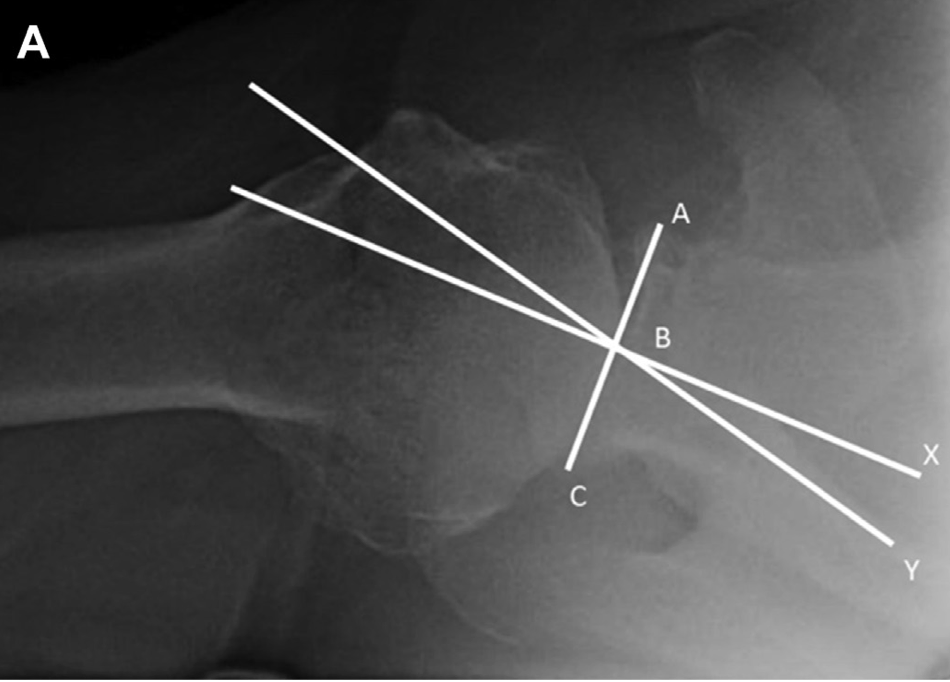

Left figure above. Assessment of preoperative glenoid retroversion. Line A-C represents the glenoid plane, which is drawn connecting the anterior (A) and posterior (C) rims of the glenoid. Line B-Y represents the scapular plane. Line B-X is the perpendicular bisector of line A-C. The retroversion of glenoid is defined as the angle between lines B-X and B-Y.
Right figure above. Assessment of preoperative subluxation. The same lines A-C and B-X are drawn. The humeral head circle is drawn with point Z at the center. Line segment D-F marks the humeral diameter, parallel to line A-C. Point E is the intersection between lines D-F and B-X. Subluxation is defined as the percentage of the humeral head posterior to line B-X, and is calculated as (E-F)/(D-F) X 100%.
At surgery, reaming of the anterior glenoid was carried out until satisfactory implant support (>80% of bony contact with the component) was achieved. There was no specific targeted amount of retroversion that was deemed acceptable.
In contrast to many other studies in which CT scans were used to measure the preoperative anatomical relationships and axillary views to make the postoperative measurements, these authors measured postoperative retroversion and subluxation in a manner identical to the preoperative measurements. As shown below.


At a mean followup of 4.2 years, the authors found no significant correlation between preoperative glenoid version or humeral head subluxation and the postoperative ASES scores.


The authors found no significant correlation between postoperative glenoid version or humeral head subluxation and the postoperative ASES scores.



There were no significant differences in preoperative or postoperative version for patients with or without glenoid lucencies.
The overall complication rate was 11.3%, including 5 periprosthetic joint infections, 3 with glenoid loosening, 2 rotator cuff failures, 2 periprosthetic fractures, 1 patient with stiffness treated with lysis of adhesions, and 1 patient with recurrent posterior instability after treatment with shoulder replacement after a locked posterior dislocation. Eleven of these patients underwent component revision. There was no observed difference between patients with or without revision surgery for either preoperative retroversion (15.2 ± 5.5 deg for failures vs. 15.3 ± 7.7 deg for non failures); or postoperative retroversion (7.1± 5.2 deg vs. 10.0 ± 6.8).
For the patients with eventual glenoid loosening, the preoperative retroversion was 15 and 17 deg in 2 of the 3 patients (third patient did not have available preoperative imaging) and the postoperative retroversion was 6, 8, and 19 deg. The preoperative subluxation was 64% and 60%, whereas postoperative subluxation was 58%, 49%, and 48%.
Comment: This study does not support the need to "correct" glenoid version to < 15 degrees in performing an anatomic total shoulder. This is consistent with the findings in Does Postoperative Glenoid Retroversion Affect the 2-Year Clinical and Radiographic Outcomes for Total Shoulder Arthroplasty?


The mean (± SD) improvement in the SST (6.7 ± 3.6; from 2.6 ± 2.6 to 9.3 ± 2.9) for the retroverted group was not inferior to that for the nonretroverted group (5.8 ± 3.6; from 3.7 ± 2.5 to 9.4 ± 3.0). The percent of maximal possible improvement (%MPI) for the retroverted glenoids (70% ± 31%) was not inferior to that for the nonretroverted glenoids (67% ± 44%). The 2-year SST scores for the retroverted (9.3 ± 2.9) and the nonretroverted glenoid groups (9.4 ± 3.0) were similar (mean difference, 0.2; 95% CI, - 1.1 to 1.4; p = 0.697). No patient in either group reported symptoms of subluxation or dislocation.


The authors concluded that in this series of TSAs, postoperative glenoid retroversion was not associated with inferior clinical results at 2 years after surgery.
This study evaluated the ability of shoulder arthroplasty using a standard glenoid component to improve patient self-assessed comfort and function and to correct preoperative humeral-head decentering on the face of the glenoid in patients with primary glenohumeral arthritis and type-B2 or B3 glenoids.
The authors identified 66 shoulders with type-B2 glenoids (n = 40) or type-B3 glenoids (n = 26) undergoing total shoulder arthroplasties with a non-augmented glenoid component inserted without attempting to normalize glenoid version and with clinical and radiographic follow-up that was a minimum of 2 years. The Simple Shoulder Test (SST) score (and standard deviation) improved from 3.2 ± 2.1 points preoperatively to 9.9 ± 2.4 points postoperatively (p < 0.001) at a mean time of 2.8 ± 1.2 years for type-B2 glenoids and from 3.0 ± 2.5 points preoperatively to 9.4 ± 2.1 points postoperatively (p < 0.001) at a mean time of 2.9 ± 1.5 years for type-B3 glenoids; these results were not inferior to those for shoulders with other glenoid types.

Postoperative glenoid version was not significantly different (p > 0.05) from preoperative glenoid version. The mean humeral-head decentering on the glenoid face was reduced for type-B2 glenoids from -14% ± 7% preoperatively to -1% ± 2% postoperatively (p < 0.001) and for type-B3 glenoids from -4% ± 6% preoperatively to -1% ± 3% postoperatively (p = 0.027). The rates of bone integration into the central peg for type-B2 glenoids (83%) and type-B3 glenoids (81%) were not inferior to those for other glenoid types.

The authors concluded that shoulder arthroplasty with a standard glenoid inserted without changing version can significantly improve patient comfort and function and consistently center the humeral head on the glenoid face in shoulders with type-B2 and B3 glenoids, achieving >80% osseous integration into the central peg. These clinical and radiographic outcomes for type- B2 and B3 glenoids were not inferior to those outcomes for other glenoid types
Long term followup of well-characterized patients treated with the different methods for managing glenoid retroversion will be required to define the relative risks, benefits, effectiveness and durability of each of them.
You can support cutting edge shoulder research that is leading to better care for patients with shoulder problems, click on this link.
Follow on twitter: https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interestShoulder arthritis - what you need to know (see this link).How to x-ray the shoulder (see this link).The ream and run procedure (see this link).The total shoulder arthroplasty (see this link).The cuff tear arthropathy arthroplasty (see this link).The reverse total shoulder arthroplasty (see this link).The smooth and move procedure for irreparable rotator cuff tears (see this link).Shoulder rehabilitation exercises (see this link).
Follow on twitter: https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/