There is increasing interest by active women in the ream and run arthroplasty for glenohumeral arthritis.
Here are some examples of highly motivated women who have made an excellent recovery from their arthritis after having a ream and run procedure.
#1. A woman black belt instructor in
shotokan karate presented 14 years ago with pain, loss of function of the left shoulder, and this x-ray.
She had a ream and run procedure.
Two years ago she presented with similar symptoms of her right shoulder and this x-ray.
She had a ream and run procedure for this shoulder.
The fourteen year followup x-rays of the left shoulder are shown below
The two year postoperative x-rays of the right shoulder are shown below.
In the video below she shows full use of her shoulders in her Karate practice.
#2. An athletic young woman in her mid 20s was diagnosed with multidirectional instability of her right shoulder. She was treated elsewhere with an arthroscopic anterior and posterior capsulorrhaphy. Three years later she had a repeat surgery after which a pain pump was used to infuse local anesthetics. Eight years later she had a subacromial decompression and biceps tenodesis. At that time glenohumeral chondromalacia was identified. The shoulder was debrided and the repair sutures removed. Five months later another subacromial decompression was performed along with a distal clavicle excision. She had persistent stiffness and pain. At the time of her presentation to us - twelve years after her first surgery - she had flexion limited to 90 degrees, pain ranging from 7-10 on a scale of 10, and reported the inability to perform any of the twelve functions of the Simple Shoulder Test.
Her radiographs showed bone on bone contact in both the AP and the axillary views as shown below, suggesting chondrolysis (noting that primary degenerative joint disease would be very unusual in such a young woman).
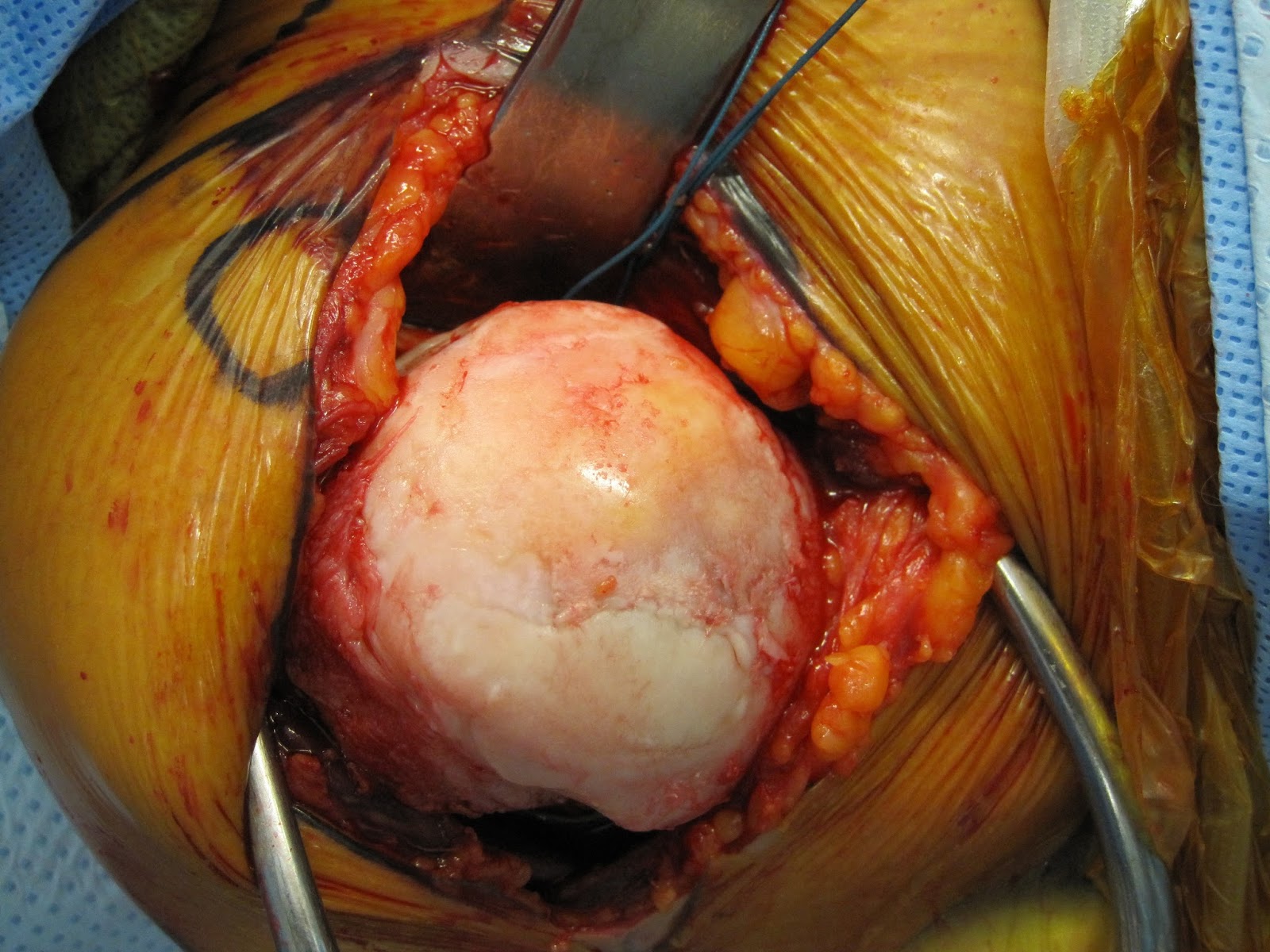
At surgery, the loss of cartilage over the humeral head was evident.
She elected to have a ream and run procedure to avoid the potential risks and limitations associated with a total shoulder arthroplasty (glenoid component wear and loosening).
Her postoperative films are shown below. Note the absence of a plastic glenoid and the absence of bone cement. Note the humeral stem was secured using impaction auto grafting with bone harvested from the humeral head.


Although her motion was improved at 6 weeks after surgery, she and her local orthopaedic surgeon decided to proceed with a manipulation under anesthesia in that she had lost some of her early range of motion
She demonstrated the highest level of dedication to her rehabilitation program, taking it to trackside. She has generously allowed us to post some of her photos here.
Here are the photos she sent in at 4 months after surgery, stating that she can now perform 8 of the 12 functions of the Shoulder Test in contrast to 0/12 before surgery.
At two years out from the procedure and fully functional as shown by these images she recently sent to us along with this message "Today is my two year anniversary of my ream and run surgery! We did it! I am so happy and proud to say that my shoulder feels better and stronger than it has in 15 years, since before my very first surgery in 2003! Thank you both from the bottom of my heart for giving me the chance at a much greater quality of life! Aloha, "
She adds "I can now perform all 12 functions of the Simple Shoulder test :) (the 8lb one is challenging but I can do it!)"




Recently she posted, "I am recently six years out from my ream and run surgery and I have to say it was one of the best decisions I’ve made. My story is a little different from some others so I wanted to share it in case it can help someone who may be on the fence. At age 23 I worked in the bars and would dislocate my shoulder so much I could Lethal Weapon it back in place myself lol. I had surgery to tighten loose tendons and ligaments. At age 26, after a bad car accident, the laxity returned. After months and months of physical therapy it was determined I needed surgery again. Following this surgery, in 2006, my surgeon put a pain pump with a catheter directly into my chest for pain management. It looked like a little battery pack. After 3 days I had a friend help me pull the catheter out of my chest, as instructed. Shortly after that surgery I knew something felt very different. Quarterly cortisone injections and 9 years of corrective surgeries including but not limited to clavicle resection, biceps tenodesis, AC joint repair, you name I feel like I had it. Not to mention the countless manipulations under anesthesia. At age 29, a different surgeon told me I had the shoulder of an 80 year old but “you’re too young for a replacement.” No one could tell me how my shoulder had gotten so bad. It got to the point it was painful moving a computer mouse. At age 34, I saw a new surgeon here in Hawaii. He knew right away what I had…Chondrolysis…from that pain pump in 2006. Chondrolysis is a severe type of shoulder arthritis in which the cartilage of the joint is abruptly lost. He referred me to the UW and at age 35 I had my ream and run. The recovery was tough but 9 years with no resolution was tougher! It’s all about Quality of Life 💕 I am so thankful and have a shoulder that I am no longer aware of every single day, a shoulder that is pain-free, and able to do all that I need it to do without hesitation. Happy I don’t do any power lifting or have a physically demanding career or anything like that but I’m 120lbs and just helped lift a gazebo roof that was at least my body weight. The r&r was the absolute best thing I ever did! I was just telling my husband that for nearly a decade I was aware of my shoulder every single day...now I’m never aware of it and haven’t been to a doctor for over three years! "
#3. A 60ish year old active woman (personal trainer for 32 years) presented with left shoulder pain and stiffness and these radiographs showing glenohumeral osteoarthritis

and posterior decentering of the humeral head on a biconcave glenoid as shown on an axillary "truth" view.
Because of her active lifestyle and to avoid the risks and limitations of a prosthetic glenoid component, she elected to have a ream and run procedure
At eight days after surgery, she sent this photo of her motion.
Shown below are her x-rays at 5 weeks and one day after surgery.
At which time she started her active motion as shown below.
She is following the program shown in this
link.
She added swimming at six weeks as shown below
A few days later
And at 4 months

#4. Here are the x-rays of an active woman in her 60s with degenerative arthritis and a Simple Shoulder Test of 5/12.After a discussion of the options and in consideration of her active lifestyle, she elected to proceed with a ream and run procedure in order to avoid the potential risks and limitations of a prosthetic glenoid component.At her six weeks check her shoulder was a bit stiff in spite of her great rehabilitative effort; she elected to have a manipulation under anesthesia and complete muscle relaxation - a full range of passive motion was achieved.Four months after the ream and run, she returned with a much improved shoulder and these x-raysNote the impaction grafted stem and the conservatively reamed glenoid, now with a radiographic joint space between it and the prosthetic humeral component.Five months after her surgery she sent this video clip of her swimming at Coogee beach, the site of the famous "shark arm case (see this link)". and kindly gave us permission to show it here.#5. A sixty six year old highly motivated woman presented with pain and stiffness of the right shoulder and these x-rays


She elected to proceed with a ream and run procedure.
Four years later she presented with pain and stiffness of her left shoulder and these x-rays.
Again, she elected the ream and run procedure.
Fourteen years after her right ream and run and ten years after her left ream and run she reported full comfortable function of both shoulders.
Her followup x-rays are shown below.
Each of these procedures was performed without a preoperative CT scan or the use of 3D preoperative planning software. A brachial plexus block was not used. The ream and run technique is shown in this link.
In thinking about these highly motivated women, the following quote, variously attributed to Hippocrates and to Osler, comes to mind, "It is far more important to know what person the disease has than what disease the person has."
You can support cutting edge shoulder research that is leading to better care for patients with shoulder problems, click on this link.
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link). How to x-ray the shoulder (see this link). The ream and run procedure (see this link). The total shoulder arthroplasty (see this link). The cuff tear arthropathy arthroplasty (see this link). The reverse total shoulder arthroplasty (see this link). The smooth and move procedure for irreparable rotator cuff tears (see this link). Shoulder rehabilitation exercises (see this link).