Surgeons want to know how the postoperative position of the humerus in relation to the scapula relates to the clinical outcome after reverse total shoulder arthroplasty (RSA).
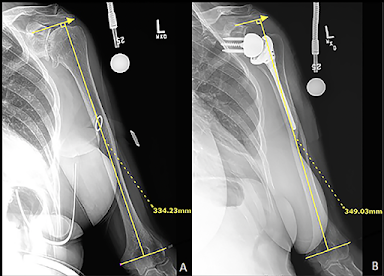
The authors of The lateralization and distalization shoulder angles are important determinants of clinical outcomes in reverse shoulder arthroplasty studied these relationships in 46 patients having RSA for cuff tear arthropathy (CTA) using measurements of the lateralization shoulder angle (LSA) and the distalization shoulder angle (DSA) as shown below. Four different implant combinations were included.


Although they found positive correlations between the LSA and the ADLER score and the Constant score, they found no significant correlations between the LSA and ASES, SST, or SSV scores.
While they found negative correlations between the DSA and the ADLER score, they found no significant correlations between the DSA and the total Constant, ASES, SST, or SSV scores.
You can support cutting edge shoulder research that is leading to better care for patients with shoulder problems, click on this link.
Follow on twitter: https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link).
Shoulder rehabilitation exercises (see this link).
More recently the authors of Lateralization and distalization shoulder angles do not predict outcome in reverse shoulder arthroplasty for cuff tear arthropathy reviewed a larger series of 630 primary RSAs for patients with CTA. Five different implants were used. The regression calculations for LSA or DSA did not reveal significant associations with any of the clinical outcomes.
In Influence of humeral lengthening on clinical outcomes in reverse shoulder arthroplasty no clear relationship between humeral lengthening and clinical outcomes was identified.
In Negligible Correlation between Radiographic Measurements and Clinical Outcomes in Patients Following Primary Reverse Total Shoulder Arthroplasty the importance of radiographic measurements and their correlation with clinical and functional outcomes following rTSA was found to be limited.
In Does glenohumeral offset affect clinical outcomes in a lateralized reverse total shoulder arthroplasty? the magnitude of lateralization did not significantly affect the clinical outcomes.
In Medialized vs. lateralized humeral implant in reverse total shoulder arthroplasty: the comparison of outcomes in pseudoparalysis with massive rotator cuff tear the postoperative active elevation range and functional outcomes were not affected by medialization or lateralization of the humeral implant.
Finally, the authors of Managing rotator cuff tear arthropathy: A role for cuff tear arthropathy hemiarthroplasty as well as reverse total shoulder arthroplasty studied the postoperative relationships in 58 patients having RSA for CTA, including:
(1) the superior/inferior position of the greater tuberosity in relation to the acromion tip
(2) the medial/lateral position of the greater tuberosity in relation to the acromion tip
(3) the superior/inferior position of the center of rotation in relation to the bony glenoid center
(4) the medial/lateral position of the center of rotation in relation to the bony glenoid center
(5) the abduction moment
(6) the distance from the center of rotation to the greater tuberosity
(7) the distance from the center of rotation to the acromion
As in the prior reports, none of these parameters were significantly associated with clinical outcome.
Comment: Factors other than postoperative radiographic parameters are responsible for the amount of improvement in patient comfort and function following RSA.
Follow on twitter: https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link).
Shoulder rehabilitation exercises (see this link).