The reverse total shoulder replacement can restore comfort and function to the arthritic shoulder combined with a massive rotator cuff tear and for failed conventional total shoulder replacement. This combination of conditions can result in major loss of stability and active motion of the shoulder. The reverse total shoulder provides stability of the shoulder joint so that the deltoid muscle can power the shoulder through a useful range of motion. In this procedure the arthritic ball is replaced by a socket fixed to the arm bone (humerus) by a stem that fits within it. A metal ball is fixed to the bone of the arthritic socket with screws. Success requires technical excellence of the surgery and a commitment to the rehabilitation program until the desired range of motion can be achieved comfortably. The figure below left shows the humeral stem, cup, and white polyethylene cup as well as the glenosphere (ball) and screws used for fixation into the scapula (shoulder blade). The figure below right is an x-ray of this prosthesis in place.

First, a review of some basics.
What Are The Key Parts Of The Normal Shoulder Joint?
The ball (humeral head) fits in the socket (glenoid) and is held there by the rotator cuff
What Is Shoulder Arthritis?
Shoulder arthritis is a condition in which degeneration, injury, inflammation or previous surgery destroys the normally smooth cartilage on the ball (humeral head-below left) and socket (glenoid-below right).
How Is Shoulder Arthritis Diagnosed?
Carefully standardized X-rays reveal the loss of the space between the humeral head and glenoid that is normally occupied by cartilage, leaving bone on bone contact.
What Is A Conventional Total Shoulder?
In a conventional total shoulder, the arthritic surface of the ball is replaced with a metal ball with a stem that is press fit in the inside of the arm bone (humerus-below left) and the socket (glenoid) is resurfaced with a high density polyethylene component (below right).
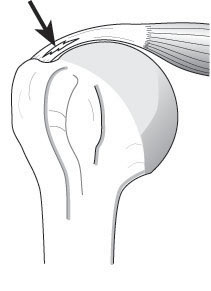
When Will A Conventional Shoulder Not Work?
When the rotator cuff is sufficiently torn that it no longer provides the necessary stability for the joint, the humeral head slides upwards. This results in slackening of the deltoid (below left) no longer able to raise the hand to carryout normal activities. A conventional shoulder cannot restore the necessary stability in this situation (below right).
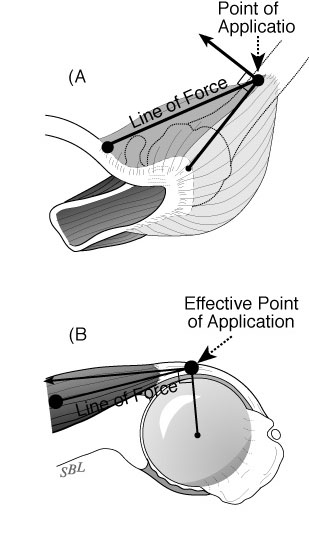
What Is A Reverse Total Shoulder?
In a reverse total shoulder the ball is located on the shoulder blade (glenoid) and the socket is located on the arm bone (humerus), exactly the opposite of the situation in a conventional total shoulder. This configuration provides stability because the muscles around the shoulder compress the ball and socket together.
How Are The Parts Of A Reverse Total Shoulder Hooked To The Bones?
The ball (glenosphere) is screwed to the bone of the shoulder blade. The cup (humeral socket) is fixed to a stem that is cemented down the inside of the arm bone (humerus).
What Is The Incision Like?
After a general or regional anesthetic, this procedure is performed through an incision between the deltoid and the pectoralis major muscles on the front of the shoulder. It includes release of adhesions and contractures and removal of bone spurs that may block range of motion. Our team of surgeons, anesthesiologists, and surgical assistants usually perform this procedure in less than two hours.
Who Should Consider A Reverse Total Shoulder?
Surgery for shoulder arthritis and rotator cuff deficiency should only be considered when the condition of the shoulder is limiting the quality of the patient’s life and after a trial of physical therapy and mild analgesics to determine if non-operative management is helpful. If severe disability persists, patients may consider the reverse total shoulder – no other surgical procedure has the ability to restore the stability needed in the absence of a functioning rotator cuff. The ideal patient is healthy, active, motivated and committed to complying with the rehabilitation program.
Who Should Probably Not Consider A Reverse Total Shoulder?
This procedure is less likely to be successful in individuals with depression or obesity. Patients who use narcotic medication or who use tobacco may have increased difficult recovering from this procedure.
What Are The Keys To Success Of A Reverse Total Shoulder?
Success requires technical excellence of the surgery and a commitment by the patient to follow the rehabilitation program prescribed by the surgeon.
How Does A Patient Prepare For A Reverse Total Shoulder?
As for all elective surgical procedures, the patient should be in the best possible physical and mental health at the time of the procedure. Any heart, lung, kidney, bladder, tooth, or gum problems should be managed before surgery. Any infection may be a reason to delay the operation. Any skin problem (acne, scratches, rashes, blisters, burns, etc) on the shoulder or arm should be resolved before surgery. The shoulder surgeon needs to be aware of all health issues, including allergies as well as the non-prescription and prescription medications being taken. For instance, aspirin and anti-inflammatory medication may affect the way the blood clots. Some of these may need to be modified or stopped around the time of surgery.
What Happens After Surgery?
The reverse total shoulder is a major surgical procedure that involves cutting of skin, tendons and bone. The pain from this surgery is managed by the anesthetic and by pain medications. Immediately after surgery, strong medications (such as morphine or Demerol) are often given by injection. Within a day or so, oral pain medications (such as hydrocodone or Tylenol with codeine) are usually sufficient. The shoulder rehabilitation program is started on the day of surgery. The patient is encouraged to be up and out of bed soon after surgery and to progressively reduce their use of pain medications. Hospital discharge usually takes place on the second or third day after surgery. The arm is kept in a sling for six weeks after the procedure to allow for healing, but the patient can use the hand for eating. Driving is not recommended during this time. Thus the patient needs to be prepared to have less arm function for the six weeks after surgery than immediately before surgery. For this reason, patients usually require some assistance with self-care, activities of daily living, shopping and driving. Management of these limitations requires advance planning to accomplish the activities of daily living during the period of recovery.
What About Rehabilitation?
After the six weeks in a sling, progressive use of the shoulder for usual daily activities is encouraged. Formal physical therapy is often not needed.
When Can Ordinary Daily Activities Be Resumed?
The reverse total shoulder is not a procedure that is designed for heavy use or sports. It is designed to help the patient regard the gentle activities of daily living. Every precaution should be taken to avoid falls on the operated shoulder.
What Problems Can Complicate A Reverse Total Shoulder And How Can They Be Avoided?
Like all surgeries, the reverse total shoulder can be complicated by infection, nerve or blood vessel injury, fracture, instability, component loosening, and anesthetic complications. Furthermore, this is a technically exacting procedure and requires an experienced surgeon to optimize the bony, prosthetic and soft tissue anatomy after the procedure. The procedure can fail if the reconstruction is too tight, too loose, improperly aligned, insecurely fixed or if unwanted bone-to-bone contact occurs.
Conclusion
Summary reverse total shoulder replacement for the arthritic shoulder combined with a massive rotator cuff tear.
The reverse total shoulder is a a technically challenging surgical procedure that can restore comfort and function to shoulders with arthritis and massive defects in the rotator cuff or in failed conventional total shoulder replacement. In the hands of an experienced surgeon, the reverse total shoulder can be an effective method for treating shoulders arthritis and severe rotator cuff deficiency. Pre-planning and persistent rehabilitation efforts will help assure the best possible result for the patient.





















































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}