
These authors created finite element reverse shoulder arthroplasty (RSA) models with varying neck-shaft angles (155°, 145°, 135°), sizes (38 mm, 42 mm), and cup depths (deep, normal, shallow) were loaded with 400 N at physiological abduction angles.
They found that the location of maximum contact stress were typically located inferomedially in the polyethylene humeral cup.
Reducing the neck-shaft angle reduced the contact area and increased maximum contact stress.
Increasing the glenosphere size increased the contact area and slightly decreased maximum contact stress.
Decreasing the cup depth reduced the contact area and increased maximum contact stress.
The authors note the tradeoff: although reducing the neck-shaft angle and cup depth can improve range of motion these changes may have negative effects on contact mechanics.
Comment: It is of interest that current practice of RSA is tending toward implant modifications that increase range of motion: reduced neck shaft angle, smaller glenosphere diameter and shallower cups, all changes that may increase the risk of cup wear.
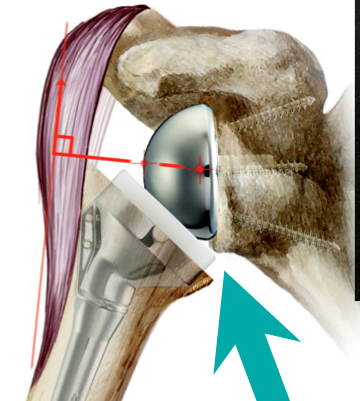
Thus in reverse total shoulder arthroplasty, design does matter. As we pointed out in a recent post and here, different component designs have different effects on the position of the center of rotation - both superiorinferiorly (which affects deltoid tension) and mediolaterally (which affects stability and the proximity of the medial aspect of the humeral component to the glenoid). The design of the component also determines the shape of the glenoid polyethylene and the varus/valgus orientation of the humeral cup. Stated simply, designs that place more polyethylene beneath the glenosphere tend to be more stable on one hand while increasing the risk of notching on the other.










Comment: It is of interest that current practice of RSA is tending toward implant modifications that increase range of motion: reduced neck shaft angle, smaller glenosphere diameter and shallower cups, all changes that may increase the risk of cup wear.
Contact between the polyethylene at the medial aspect of the humeral cup and the scapula is bad; it can give rise to (1) scapula notching, (2) instability from levering of the humeral component away from the glenoid, (3) limited range of motion and (4) destruction of the polyethylene as shown below and as described here and here with the production of polyethylene debris.


Consider the figures below, each of which was taken from the website of a vendor of a reverse total shoulder (please recall that we have no financial relationships with any company making orthopaedic implants). Note the relationship of the center of rotation of the glenoid component to the proximity of the medial aspect of the humeral cup to the scapula. Interestingly some illustrations show the arm in abduction, which can mask the proximity when the arm is adducted.



Some authors have advocated modifying the medial/lateral position of the glenosphere by the insertion of a bone graft with the explicit goal of minimizing the risk of notching as shown below.

Some prosthetic designs accomplish the same effect by adding a neck to the glenosphere.

This change in design has an effect on the medial/lateral position of the center of rotation and adding distance between the humeral component and the scapula.
It is important to keep an eye on the mechanisms of reverse total shoulder failure as posted here and here and here and here
Our current approach to reverse total shoulder arthroplasty is shown in this post.
===
Use the "Search" box to the right to find other topics of interest to you.
You may be interested in some of our most visited web pages including:shoulder arthritis, total shoulder, ream and run, reverse total shoulder, CTA arthroplasty, and rotator cuff surgery as well as the 'ream and run essentials'
You may be interested in some of our most visited web pages including:shoulder arthritis, total shoulder, ream and run, reverse total shoulder, CTA arthroplasty, and rotator cuff surgery as well as the 'ream and run essentials'