
These authors point out that many new designs of humeral components are 'stemless' with the goal of being "canal-sparing", allowing restoration of the glenohumeral center of rotation independently from the shaft, and avoiding stem-related complications.
They systematically reviewed the literature for studies of currently available canal-sparing stemless shoulder arthroplasty systems, finding 11 studies (929 cases) published between 2010 and 2016. The rates of humeral component-related complications ranged between 0 and 7.9 %.
through the use of metaphyseal fixation.
While there is no question that good results have been reported with these prostheses, we are unaware of evidence that patients with stemless prostheses achieve clinical outcomes that are superior to those seen with conventional prostheses. Furthermore, clinical experience indicates that stemless prostheses have their own learning curve and set of potential problems of fixation and positioning as shown in the films below.


We find in the great majority of cases, the proposed advantages of canal sparing prostheses can be achieved with impaction grafting of a thin stem: preservation of humeral bone stock for potential revisions, performance of anatomic reconstruction regardless of posterior offset in anatomic arthroplasty, facilitating arthroplasty in cases of humeral deformity, prevention of malpositioning, and avoiding periprosthetic fractures.
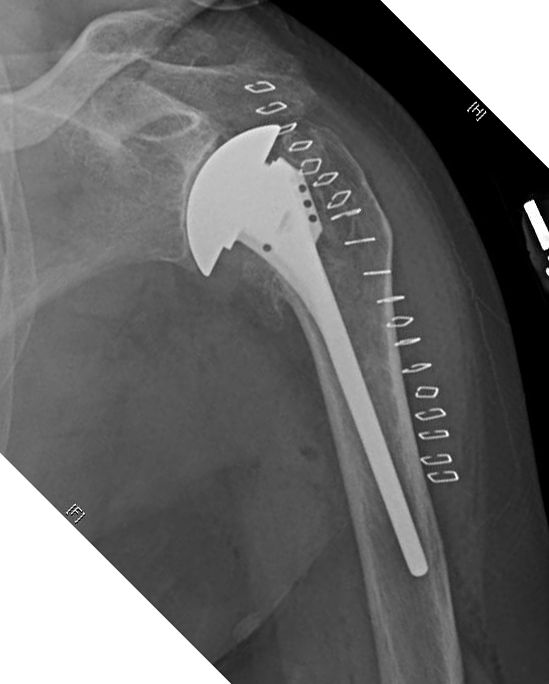
The variations of intramedullary anatomy are recognized

and managed by impacting humeral autograft into the canal, 'reinvesting' the patients own bone in strengthening the humeral shaft.

This approach enables precise positioning of a humeral component with a smaller stem, secure safe fixation, and ease of prosthesis exchange should revision become necessary. Note the absence of cortical contact with the tip of the prosthesis.


It also allows the use of an anteriorly eccentric humeral head to manage posterior instability, a modification not possible with stemless implant.


It is apparent that management of a post traumatic arthritic shoulder can be complicated if the humerus is malunited in varus.

because normal positioning of the humeral component would conflict with the cuff attachment to the tuberosity.

In these cases it is possible to use impaction grafting to fix a small stemmed humeral prosthesis in an amount of varus that matches the deformity, so that the humeral head is positioned in the center of the glenoid. In the case below, the fixation of the humeral component was robust - more than what we could have achieved with a stemless prosthesis.
Here's another humeral deformity managed with a thin stem and impaction grafting.


Different approaches to 'sparing' the canal.
===
Consultation for those who live a distance away from Seattle.
Click here to see the new Shoulder Arthritis Book.
Click here to see the new Rotator Cuff Book
Click here to see the new Shoulder Arthritis Book.
Click here to see the new Rotator Cuff Book
Use the "Search" box to the right to find other topics of interest to you.
You may be interested in some of our most visited web pages including:shoulder arthritis, total shoulder, ream and run, reverse total shoulder, CTA arthroplasty, and rotator cuff surgery as well as the 'ream and run essentials'
See from which cities our patients come.
See the countries from which our readers come on this post.
You may be interested in some of our most visited web pages including:shoulder arthritis, total shoulder, ream and run, reverse total shoulder, CTA arthroplasty, and rotator cuff surgery as well as the 'ream and run essentials'
See from which cities our patients come.
See the countries from which our readers come on this post.