This article presents a review of patients having total shoulder arthroplasty using the combination of a high-density polyethylene glenoid component, polymethyl methacrylate bone cement, and a porous metal implant to address glenoid retroversion.

The study included 66 patients (23 women and 43 men, aged 42-85 years)
All but 4 glenoids were within the target range (less than 10 retroversion), and only 2 glenoid components were implanted with more than 15 degrees from neutral version.
Patients underwent preoperative 3-dimensional (3D) templating; based on that planning, patients received either a 15 or 30 degree wedge secured by screws to the native glenoid to address glenoid retroversion before a standard glenoid component was implanted using bone cement.
49 shoulders with a follow-up of greater than 24 months showed improved outcome scores.
Apart from 1 infection at 18 months postoperatively and 1 minor peg perforation, there were no complications, hardware failures, implant displacements, significant lucency, or posterior resubluxations.
Postoperative plain films showed incorporation of the wedge augment, with change in glenoid retroversion from a median of 22 degrees (13 to 46) to a median of 4 degrees (17 to anteversion 16).
Comment: This is an interesting approach to modification of gleonoid version with a posterior metal wedge and a standard polyethylene glenoid component in contrast to a posteriorly augmented polyethylene glenoid component.

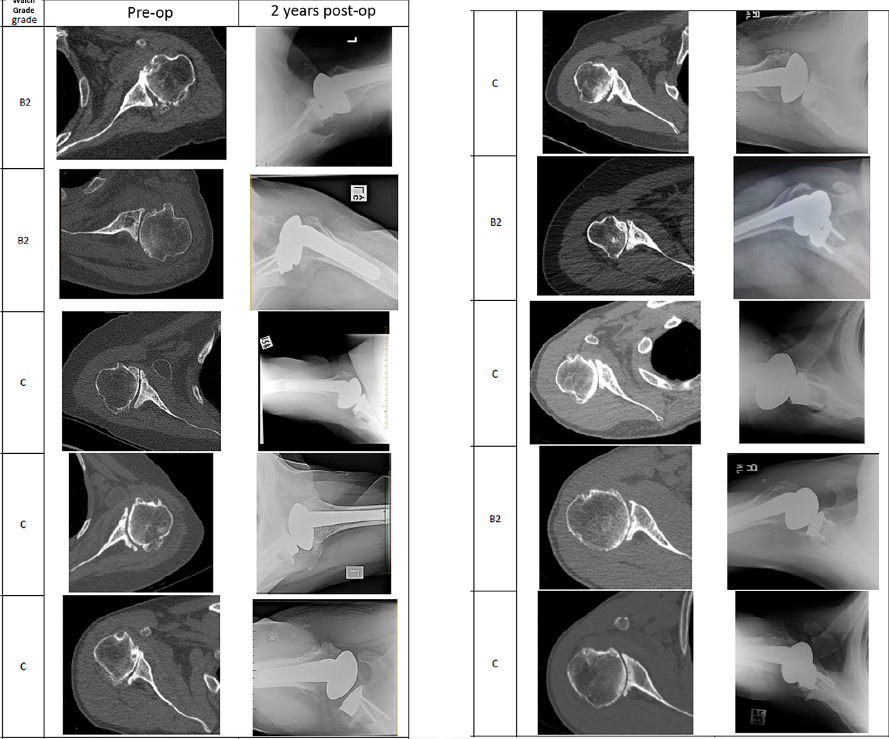
For us, the question remains, "how clinically important is it to change the glenoid version in performing a total shoulder in cases such as those shown below"?




Especially when the humeral head is centered in the glenoid concavity.
The approach in this article can be compared to that used in another recent publication:
Does Postoperative Glenoid Retroversion Affect the 2-Year Clinical and Radiographic Outcomes for Total Shoulder Arthroplasty?In a population of patients undergoing TSA in whom no specific efforts were made to change the version of the glenoid, these authors asked whether at 2 years after surgery patients having glenoid components implanted in 15° or greater retroversion had (1) less improvement in the Simple Shoulder Test (SST) score and lower SST scores; (2) higher percentages of central peg lucency, higher Lazarus radiolucency grades, higher mean percentages of posterior decentering, and more frequent central peg perforation; or (3) a greater percentage having revision for glenoid component failure compared with patients with glenoid components implanted in less than 15° retroversion. They examined the records of 201 TSAs performed using a standard all-polyethylene pegged glenoid component

inserted after conservative glenoid reaming without specific attempt to modify preoperative glenoid version.

Of these, 171 (85%) patients had SST scores preoperatively and between 18 and 36 months after surgery. Ninety-three of these patients had preoperative radiographs in the database and immediate postoperative radiographs and postoperative radiographs taken in a range of 18 to 30 months after surgery. Twenty-two patients had radiographs that were inadequate for measurement at the preoperative, immediate postoperative, or latest followup time so that they could not be included. In comparison to those included in the analysis, the excluded patients did not have substantially different mean age, sex distribution, time of followup, distribution of diagnoses, American Society of Anesthesiologists class, alcohol use, smoking history, BMI, history of prior surgery or preoperative glenoid version. They analyzed the two year outcomes in the remaining 71 TSAs, comparing the 21 in the retroverted group (the glenoid component was implanted in 15° or greater retroversion (mean ± SD, 20.7° ± 5.3°)) with the 50 in the non-retroverted group ( the glenoid component was implanted in less than 15° retroversion (mean ± SD, 5.7° ± 6.9°)).
The mean (± SD) improvement in the SST (6.7 ± 3.6; from 2.6 ± 2.6 to 9.3 ± 2.9) for the retroverted group was not inferior to that for the nonretroverted group (5.8 ± 3.6; from 3.7 ± 2.5 to 9.4 ± 3.0). The percent of maximal possible improvement (%MPI) for the retroverted glenoids (70% ± 31%) was not inferior to that for the nonretroverted glenoids (67% ± 44%). The 2-year SST scores for the retroverted (9.3 ± 2.9) and the nonretroverted glenoid groups (9.4 ± 3.0) were similar (mean difference, 0.2; 95% CI, - 1.1 to 1.4; p = 0.697). No patient in either group reported symptoms of subluxation or dislocation. The radiographic results for the retroverted glenoid group were similar to those for the nonretroverted group with respect to central peg lucency (four of 21 [19%] versus six of 50 [12%]; p = 0.436; odds ratio, 1.7; 95% CI, 0.4-6.9), average Lazarus radiolucency scores (0.5 versus 0.7, Mann-Whitney U p value = 0.873; Wilcoxon rank sum test W = 512, p value = 0.836), and the mean percentage of posterior humeral head decentering (3.4% ± 5.5% versus 1.6% ± 6.0%; p = 0.223). The percentage of patients with retroverted glenoids undergoing revision (0 of 21 [0%]) was not inferior to the percentage of those with nonretroverted glenoids (three of 50; [6%]; p = 0.251).
The authors concluded that in this series of TSAs, postoperative glenoid retroversion was not associated with inferior clinical results at 2 years after surgery.
==
To see a YouTube of our technique for total shoulder arthroplasty, click on this link.
===
How you can support research in shoulder surgery Click on this link.
To see our new series of youtube videos on important shoulder surgeries and how they are done, click here.
Use the "Search" box to the right to find other topics of interest to you.
You may be interested in some of our most visited web pages arthritis, total shoulder, ream and run, reverse total shoulder, CTA arthroplasty, and rotator cuff surgery as well as the 'ream and run essentials'
The mean (± SD) improvement in the SST (6.7 ± 3.6; from 2.6 ± 2.6 to 9.3 ± 2.9) for the retroverted group was not inferior to that for the nonretroverted group (5.8 ± 3.6; from 3.7 ± 2.5 to 9.4 ± 3.0). The percent of maximal possible improvement (%MPI) for the retroverted glenoids (70% ± 31%) was not inferior to that for the nonretroverted glenoids (67% ± 44%). The 2-year SST scores for the retroverted (9.3 ± 2.9) and the nonretroverted glenoid groups (9.4 ± 3.0) were similar (mean difference, 0.2; 95% CI, - 1.1 to 1.4; p = 0.697). No patient in either group reported symptoms of subluxation or dislocation. The radiographic results for the retroverted glenoid group were similar to those for the nonretroverted group with respect to central peg lucency (four of 21 [19%] versus six of 50 [12%]; p = 0.436; odds ratio, 1.7; 95% CI, 0.4-6.9), average Lazarus radiolucency scores (0.5 versus 0.7, Mann-Whitney U p value = 0.873; Wilcoxon rank sum test W = 512, p value = 0.836), and the mean percentage of posterior humeral head decentering (3.4% ± 5.5% versus 1.6% ± 6.0%; p = 0.223). The percentage of patients with retroverted glenoids undergoing revision (0 of 21 [0%]) was not inferior to the percentage of those with nonretroverted glenoids (three of 50; [6%]; p = 0.251).
The authors concluded that in this series of TSAs, postoperative glenoid retroversion was not associated with inferior clinical results at 2 years after surgery.
==
To see a YouTube of our technique for total shoulder arthroplasty, click on this link.
===
How you can support research in shoulder surgery Click on this link.
To see our new series of youtube videos on important shoulder surgeries and how they are done, click here.
Use the "Search" box to the right to find other topics of interest to you.
You may be interested in some of our most visited web pages arthritis, total shoulder, ream and run, reverse total shoulder, CTA arthroplasty, and rotator cuff surgery as well as the 'ream and run essentials'