
Four Ps determine the outcome: problem (diagnosis), patient (demographics), physician (surgeon characteristics, including case volume), and procedure.
These authors examined the effect of surgeon or hospital shoulder arthroplasty volume on perioperative metrics related to shoulder hemiarthroplasty, total shoulder arthroplasty, and reverse shoulder arthroplasty in a multicenter shoulder arthroplasty registry study of 1176 primary shoulder arthroplasty cases.
Surgeon volume was based on a simple tertial cut of the distribution of cases performed by individual surgeons, i.e. for each procedure one third of the surgeons were in each group, regardless of the number of cases in each tertian.
For hemiathroplasty, the tertial cutoffs were fewer than 2 cases per year for low-volume practitioners, 2 to 4 cases a year for medium-volume surgeons, and more than 4 cases annually for high-volume surgeons.
For total shoulder arthroplasty The tertial cutoffs were fewer than 5 cases per year for low-volume practitioners, between 6 and 15 cases a year for the medium-volume group, and more than 15 cases annually for higher volume surgeons.
For reverse total shoulder Low-volume surgeons performed 4 or fewer cases per year; medium volume was considered 5 to 8 cases a year; and higher volume practitioners performed 9 or more procedures annually. We were not clear whether the surgical volume was determined as the total number of cases performed by each surgeon over the period of the study divided by the number of years of the study, or, preferably, if the surgeon volume was the number of cases done by the surgeon in the year that the arthroplasty was performed.
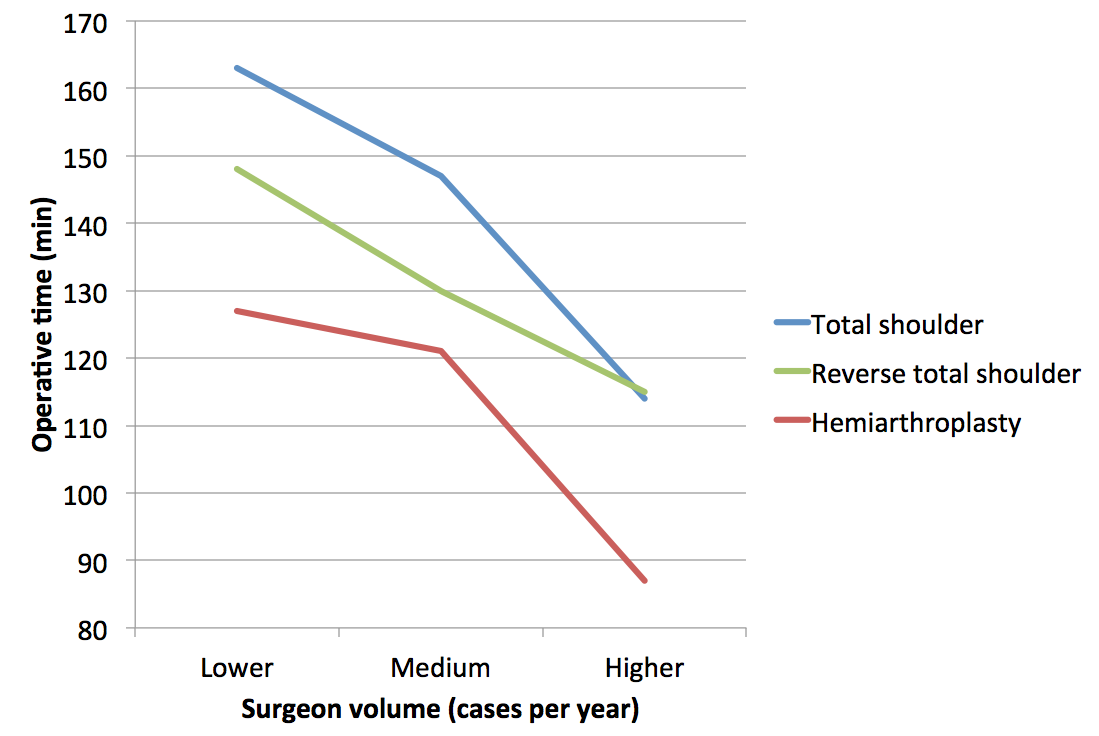
The authors found that surgeon volume was inversely correlated with length of stay for hemiarthroplasty and total shoulder arthroplasty and with blood loss and operative time for all 3 procedures.
Hospital volume was inversely correlated with length of stay for hemiarthroplasty, with blood loss for total and reverse shoulder arthroplasty, and with operative time for all 3 procedures.
High-volume surgeons performed shoulder arthroplasty 30 to 50 minutes faster than low-volume surgeons did.
The authors concluded that higher surgeon and hospital case volumes led to improved perioperative metrics with all three of these shoulder arthroplasty procedures.
Comment: Operative time is more than about speed. Longer surgical times mean more time under anesthesia, more time at risk for contamination, more risk of blood loss and nerve injury.
Higher surgeon case volume may reflect the efficiencies of the surgical team, more astute patient selection, and more organized pre and post surgical care.
===
Consultation for those who live a distance away from Seattle.
Click here to see the new Rotator Cuff Book
To see the topics covered in this Blog, click here
Use the "Search" box to the right to find other topics of interest to you.
You may be interested in some of our most visited web pages including:shoulder arthritis, total shoulder, ream and run, reverse total shoulder, CTA arthroplasty, and rotator cuff surgery as well as the 'ream and run essentials'
You may be interested in some of our most visited web pages including:shoulder arthritis, total shoulder, ream and run, reverse total shoulder, CTA arthroplasty, and rotator cuff surgery as well as the 'ream and run essentials'