
Clinical effectiveness and cost-effectiveness of open and arthroscopic rotator cuff repair [the UK Rotator Cuff Surgery (UKUFF) randomised trial].
First, thanks to our past fellow, Mac McElvany, for bringing this Level I study to our attention.
The authors point out that uncertainty exists regarding the best management of patients with degenerative tears of the rotator cuff in patients aged ≥ 50 years.
They conducted a two parallel-group randomised controlled trial involving 19 teaching and district general hospitals in the UK with 273 patients, comparing arthroscopic surgery and open rotator cuff repair. Tears were small or medium in size <3 cm) in 75% of the shoulders. The average age of the patients was 63 years. 40% were women. Patients had symptoms for an average of 2.5 years prior to treatment.
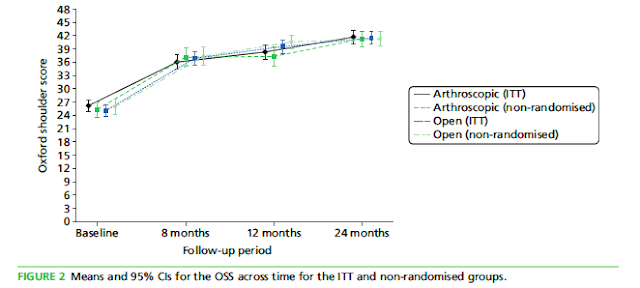
The questionnaire response rate was > 86%.For both the intention-to-treat analysis and the per protocol analysis, there was no statistical difference between the groups: the mean Oxford Shoulder Score (OSS) improved from 26.3 [standard deviation (SD) 8.2] at baseline to 41.7 (SD 7.9) at 24 months for arthroscopic surgery and from 25.0 (SD 8.0) at baseline to 41.5 (SD 7.9) at 24 months for open surgery. Total quality-adjusted life-years accrued at 24 months averaged 1.34 (SD 0.05) in the arthroscopic repair group and 1.35 (SD 0.05) in the open repair group, a non-significant difference of 0.01 (95% CI -0.11 to 0.10).

Comment: As in the preceding post, these authors have studied the most common type of cuff defect: degenerative (as opposed to traumatic) see this link. These results fail to show an advantage of arthroscopic over open repair. Once again the retear rate after repair of relatively small degenerative tears is seen to be high. Mindful of results like these, we continue to consider the 'smooth and move' procedure (see link) in the management of atraumatic tears.
At 8 months, 77% of participants reported that shoulder problems were much or slightly better, and at 24 months this increased to 85%.
There were no significant differences in mean cost between the arthroscopic group and the open repair group for any of the component resource-use categories, nor for the total follow-up costs at 24 months.
The rate of re-tear was not significantly different across the randomised groups (46.4% and 38.6% for arthroscopic and open surgery, respectively). The participants with tears that were impossible to repair had the lowest OSSs, the participants with re-tears had slightly higher OSSs and the participants with healed repairs had the most improved OSSs.


Comment: As in the preceding post, these authors have studied the most common type of cuff defect: degenerative (as opposed to traumatic) see this link. These results fail to show an advantage of arthroscopic over open repair. Once again the retear rate after repair of relatively small degenerative tears is seen to be high. Mindful of results like these, we continue to consider the 'smooth and move' procedure (see link) in the management of atraumatic tears.
===
Consultation for those who live a distance away from Seattle.Click here to see the new Rotator Cuff Book
To see the topics covered in this Blog, click here
Use the "Search" box to the right to find other topics of interest to you.
You may be interested in some of our most visited web pages including:shoulder arthritis, total shoulder, ream and run, reverse total shoulder, CTA arthroplasty, and rotator cuff surgery as well as the 'ream and run essentials'
You may be interested in some of our most visited web pages including:shoulder arthritis, total shoulder, ream and run, reverse total shoulder, CTA arthroplasty, and rotator cuff surgery as well as the 'ream and run essentials'