
A recent article Biomechanical Evaluation of Subscapularis Peel Repairs Augmented with the Long Head of Biceps Tendon for Anatomic Total Shoulder Arthroplasty prompted some discussion of subscapularis management in shoulder arthroplasty.
These authors suggest that the long head of the biceps tendon (LHBT) may offer an "efficient and cheap autograft" for the augmentation of the subscapularis repair during an anatomic shoulder arthroplasty. In a cadaver study, they compared a "standard" subscapularis peel repair (using only three sutures) to two methods of subscapularis peel repair augmented with the LHBT.

They found no significant differences in the cyclic displacement between the three techniques in the superior, middle, or inferior portion of the subscapularis repair. The augmented repairs demonstrated significantly greater load to failure compared to the "traditional repair".
Comment: We prefer to preserve the long head biceps tendon at anatomic shoulder arthroplasty (unless it is severely frayed or unstable) because of its stabilizing effect (see this link). Thus the sacrifice of the biceps with the idea of reinforcing the subscapularis repair is unattractive.
The three suture repair used in this study is not representative of our standard subscapularis repair, which includes six tendon to bone sutures - the most important of which is the "mother stitch. We usually reinforce the upper aspect of the subscapularis repair with several sutures in the rotator interval.
In thousands of anatomic arthroplasties, we have noted minimal problems with subscapularis failure using the technique described below.
Take down and repair
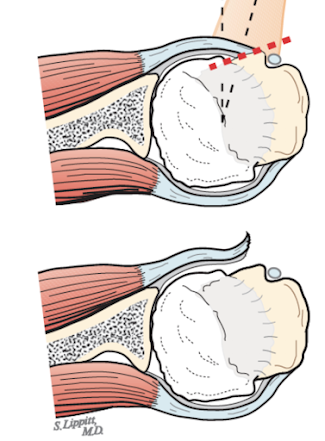
Our approach includes takedown using a careful subscapularis peel, keeping the subjacent capsule intact to the tendon.
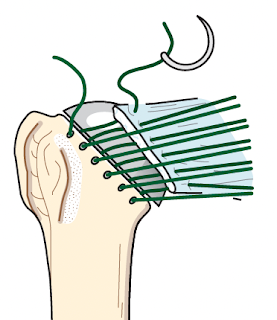
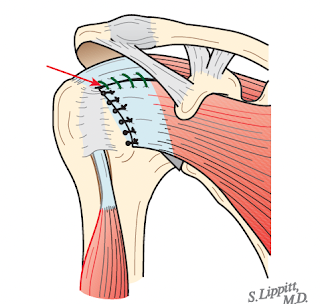
After the arthroplasty, the subscapularis tendon and subjacent capsule are repaired to the humerus using at least 6 sutures passed through secure drill holes at the margin of the humeral head cut.


This repair can be reinforced with a rotator interval plication.



You can support cutting edge shoulder research that is leading to better care for patients with shoulder problems, click on this link.
Follow on twitter: https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interestShoulder arthritis - what you need to know (see this link).How to x-ray the shoulder (see this link).The ream and run procedure (see this link).The total shoulder arthroplasty (see this link).The cuff tear arthropathy arthroplasty (see this link).The reverse total shoulder arthroplasty (see this link).The smooth and move procedure for irreparable rotator cuff tears (see this link).
Follow on twitter: https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Shoulder rehabilitation exercises (see this link).