
The authors of Reverse shoulder arthroplasty with and without latissimus and teres major transfer for patients with combined loss of elevation and external rotation: a prospective, randomized investigation sought to compare RSA outcomes in patients with rotator cuff tear arthropathy and CLEER in a randomized controlled study using RSAs without (below left) and with (below right) LD-TM tendon transfer using implants that lateralized the greater tuberosity.

{kind=link}
The primary outcome measure was the two year postoperative Activities of Daily Living and External Rotation (ADLER) score as described by the authors of Modified latissimus dorsi and teres major transfer through a single delto-pectoral approach for external rotation deficit of the shoulder: as an isolated procedure or with a reverse arthroplasty

Secondary outcome measures included the Disabilities of the Arm, Shoulder and Hand (DASH) score, American Shoulder and Elbow Surgeons (ASES) score, and Simple Shoulder Test (SST) score.
Both the treatment and control groups showed significant improvements in the ability to perform activities of daily living requiring active external rotation measured by the ADLER score postoperatively. No significant differences in the ADLER, DASH, ASES, or SST score were found between the 2 groups at final follow-up even though resolution of the Hornblower sign occurred postoperatively in 58% of patients in the control group and 73% of those in the treatment group.



In their series the ADLER score started lower (7) than the other series above and improved to 25. No control group was included.

They compared a latissimus dorsi transfer (LDT) group with a historical control group having no transfer (NT) with similar age, sex distributions, and follow-up duration.
Baseline measures were similar, except for the LDT group having slightly less active ER (-8 ⁰ vs 0⁰).
No differences were found between groups at baseline, final follow-up, or magnitude of change for ASES, VAS pain, and SSV scores. All postoperative ROM measures including aER were similar, except for a slight improvement in active internal rotation in the NT group.
Comment: From the foregoing it is apparent that a number of factors may determine whether latissimus transfer without or with teres major transfer are likely to benefit the patient enough to offset the risks of nerve injury, increased surgical time, the risk of compromising active internal rotation, and the more demanding post operative rehabilitation requirements,.

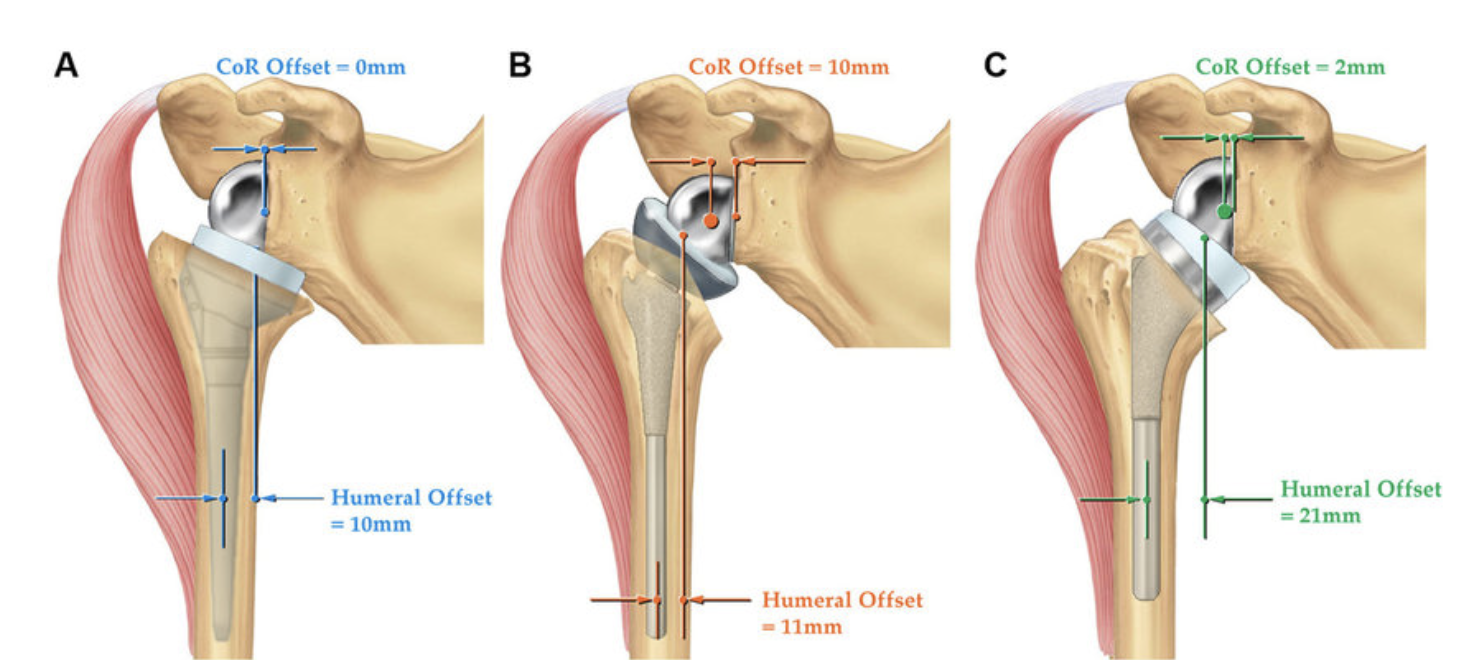
These factors might include (1) the severity of the preoperative external rotation deficit, (2) the degree to which the implant changes the line of pull of the deltoid, (3) whether both the latissimus and the teres major are transferred, and the degree to which the greater tuberosity and center of rotation are medialized or lateralized by the prosthetic implant.
The studies published to this point include a small number of patients. Controlled clinical research with a substantially larger case volume will be required to evaluate these and other factors that determine the outcome for the patient with external rotation deficits having a reverse total shoulder.
It may be that patients with functionally severe preoperative limitation of external rotation having reverse total shoulder with a medialized center of rotation and humeral offset may benefit from these tendon transfers.
Follow on twitter: https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link).
Shoulder rehabilitation exercises (see this link).