
Documenting the preoperative loss of passive range of motion (stiffness) in different directions indicates the type and severity of the limitation of motion (see these drawings by Steve Lippitt).
Flexion

Abduction

External rotation with the arm at the side

External rotation with the arm abducted

Internal rotation with the arm abducted

Reach up the back (the posterior segment that can be reached by the thumb)

and cross body adduction (the distance between the antecubital fossa and the contralateral acromion note the two-headed arrows).

Stiffness of the arthritic shoulder can be caused by muscle and capsular contracture,

osteophytes blocking motion


irregular joint surfaces,

bony deformities

prior surgical procedures

and scarring in the humeroscapular motion interface

It is often worthwhile to offer the patient with a stiff arthritic shoulder a trial of gentle stretching exercises for two reasons: (1) it may substantially improve their comfort and function and (2) it familiarizes them with the exercises that will be part of their postoperative recovery if they proceed with surgery. See Essential Shoulder Exercises.
Our approach to anatomic shoulder arthroplasty is shown here.
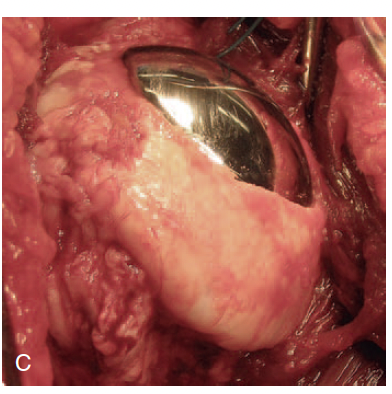
Surgical management of stiffness begins with the approach, including a 360 degree release of the subscapularis, which is often tethered

and release of the contracted capsule while protecting the axillary nerve (yellow)

With the trial components in place, the 40, 50, 60 rules can be useful targets for achieving a flexible and stable arthroplasty:
40 degrees of external rotation with the subscapularis approximated to the lesser tuberosity

50% translation on posteriorly directed loading of the proximal humerus

60 degrees of internal rotation with the arm in 90 degrees of abduction

The tightness/laxity of the shoulder can be adjusted by selecting the thickness of the humeral component that provides the desired mobility and stability.

Important causes of stiffness after an anatomic shoulder arthroplasty include
Overstuffing - too much component volume for the space available in the joint (similar to the scene in Alice in Wonderland when Alice eats a cake that makes her grow excessively).

Overstuffing can result from an inadequate humeral neck cut

from an excessively large humeral component

from a too thick glenoid component

from failure to seat the humeral component fully

from inserting the component in varus

from failure resect osteophytes at Pooh Corner

posteriorly, resulting in open booking when the arm is externally rotated

or globally

The authors of Clinical Outcomes of Anatomic Versus Reverse Total Shoulder Arthroplasty in Primary Osteoarthritis with Preoperative Rotational Stiffness and an Intact Rotator Cuff: A Case Control Study compared clinical outcomes of anatomic (aTSA) and reverse (rTSA) total shoulders performed in stiff versus non-stiff shoulders with rotator cuff intact (RCI) glenohumeral osteoarthritis (GHOA). The indications for choosing an aTSA or a rTSA are not specified. The techniques for addressing shoulder stiffness were not reported.
They defined preoperative stiffness as external rotation ≤0 degrees. They conducted a retrospective review of 1608 aTSAs and 600 rTSAs performed for RCI GHOA.
They found that patients with limited preoperative ER and RCI GHOA had lower postoperative ROM compared with non-stiff shoulders when treated with either aTSA or rTSA. Stiff shoulders treated with aTSA had better postoperative IR and ER compared to a matched cohort of stiff shoulders treated with rTSA. All groups, regardless of preoperative stiffness, had similar postoperative clinical outcome scores. They concluded that preoperative limitation in passive ER does not appear to be a limitation to utilizing aTSA in patients with RCI GHOA.
You can support cutting edge shoulder research that is leading to better care for patients with shoulder problems, click on this link.
Follow on twitter: https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link).
Shoulder rehabilitation exercises (see this link).

and release of the contracted capsule while protecting the axillary nerve (yellow)

With the trial components in place, the 40, 50, 60 rules can be useful targets for achieving a flexible and stable arthroplasty:
40 degrees of external rotation with the subscapularis approximated to the lesser tuberosity

50% translation on posteriorly directed loading of the proximal humerus

60 degrees of internal rotation with the arm in 90 degrees of abduction

The tightness/laxity of the shoulder can be adjusted by selecting the thickness of the humeral component that provides the desired mobility and stability.

Important causes of stiffness after an anatomic shoulder arthroplasty include
Overstuffing - too much component volume for the space available in the joint (similar to the scene in Alice in Wonderland when Alice eats a cake that makes her grow excessively).

Overstuffing can result from an inadequate humeral neck cut

from an excessively large humeral component

from a too thick glenoid component

from failure to seat the humeral component fully

from inserting the component in varus

from failure resect osteophytes at Pooh Corner

posteriorly, resulting in open booking when the arm is externally rotated

or globally
The authors of Clinical Outcomes of Anatomic Versus Reverse Total Shoulder Arthroplasty in Primary Osteoarthritis with Preoperative Rotational Stiffness and an Intact Rotator Cuff: A Case Control Study compared clinical outcomes of anatomic (aTSA) and reverse (rTSA) total shoulders performed in stiff versus non-stiff shoulders with rotator cuff intact (RCI) glenohumeral osteoarthritis (GHOA). The indications for choosing an aTSA or a rTSA are not specified. The techniques for addressing shoulder stiffness were not reported.
They defined preoperative stiffness as external rotation ≤0 degrees. They conducted a retrospective review of 1608 aTSAs and 600 rTSAs performed for RCI GHOA.
They found that patients with limited preoperative ER and RCI GHOA had lower postoperative ROM compared with non-stiff shoulders when treated with either aTSA or rTSA. Stiff shoulders treated with aTSA had better postoperative IR and ER compared to a matched cohort of stiff shoulders treated with rTSA. All groups, regardless of preoperative stiffness, had similar postoperative clinical outcome scores. They concluded that preoperative limitation in passive ER does not appear to be a limitation to utilizing aTSA in patients with RCI GHOA.
You can support cutting edge shoulder research that is leading to better care for patients with shoulder problems, click on this link.
Follow on twitter: https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link).
Shoulder rehabilitation exercises (see this link).