
The authors of Incidence of Primary Anatomic and Reverse Total Shoulder Arthroplasty in Patients Less than 50 Years of Age & High Early Revision Risk sought to investigate the incidence of primary anatomic total shoulder arthroplasty (TSA) and reverse shoulder arthroplasty (RSA), rate of revision within one year, and determine the associated economic burden in patients <50 years.

They found that the incidence of shoulder arthroplasty in patients <50 years old increased from 2.21 to 2.5 per 100,000 patients from 2017-2018.
In these patients the overall revision rate was 3.9% with a mean time to revision of 96.3 days. The one-year revision rate was higher in more recently performed arthroplasties (3.5% for procedures performed in 2017 and 4.4% for procedures performed in 2018).
The revision rates where higher for procedures performed in the Midwest (5.6%) and South (4.4%) than in the Northeast (1.6%) and West (1.4%).
Diabetes and female sex were significant risk factors for revision.
Surgeries performed in patients <40 years cost more than those performed in patients aged 40-50 years for both primary and revision cases.
The one-year revision rate was 3.1% for anatomic TSA and 6.8% for RSA for these patients under 50 years of age. The authors noted that young patients receiving RSA were not only more likely to undergo revision, but were also subject to greater financial, societal, and productivity costs than patients receiving anatomic TSA.
The one-year revision rate was 3.1% for anatomic TSA and 6.8% for RSA for these patients under 50 years of age. The authors noted that young patients receiving RSA were not only more likely to undergo revision, but were also subject to greater financial, societal, and productivity costs than patients receiving anatomic TSA.
Comment: In this study of one year revision rates, the average time to revision was three months. Things will get worse from that point on. As shown in the chart below from the Australian Orthopaedic Association, the revision rate at three months represents but a fraction of the longer term revision rate. 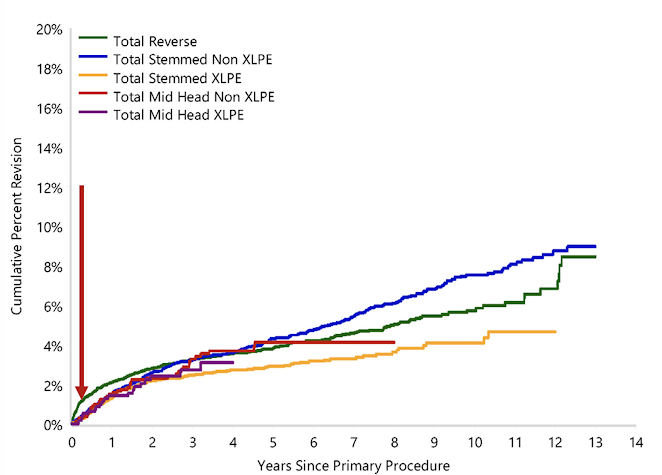
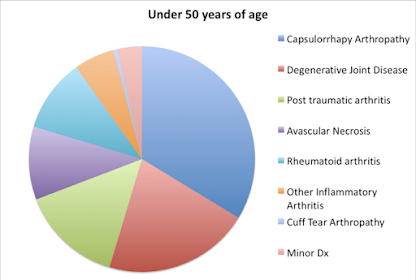
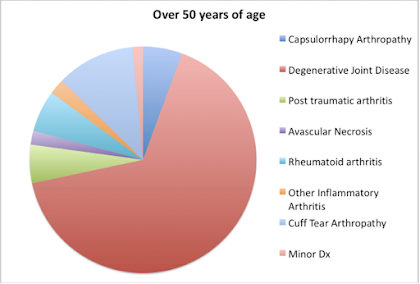
As pointed out in a prior post, the reported outcomes of shoulder arthroplasty in patients under the age of fifty years are worse than those in patients over fifty. While a number of factors, such as differences in activity level, patient longevity, and differences in expectations, have been proposed as the reason for this difference, the authors of Comparison of Patients Undergoing Primary Shoulder Arthroplasty Before and After the Age of Fifty explored the possibility that patients under fifty years of age had differences in their pre-arthroplasty self-assessed comfort and function, sex distribution, and specific type of arthritis in comparison to their more senior counterparts. Patients under the age of fifty years were not more likely than those over fifty to be female or to have a lower prearthroplasty self-assessed comfort and function score. However, they did have more complex pathological conditions, such as capsulorrhaphy arthropathy (arthritis after surgery for instability), rheumatoid arthritis, and posttraumatic arthritis. Only 21% of the younger patients had primary degenerative joint disease, whereas 66% of the older patients had that diagnosis.
They suggested that the pathoanatomy in these younger patients can complicate the surgery, the rehabilitation and the outcome of the shoulder arthroplasty. The preoperative diagnosis may have at least as much influence on the outcome of the procedure as does the age of the patient.
Recently, the authors of A History of Shoulder Instability is More Common in Young Patients Undergoing Total Shoulder Arthroplasty sought to evaluate whether a history of shoulder instability was more common in patients under 50 years old undergoing TSA. They identified 489 patients undergoing primary TSA within the Military Health System.
Patients under 50 years old were matched 1:2 with patients 50 years and older based on sex, race, and military status; the final study population comprised 240 patients.
The groups differed significantly in type of shoulder arthritis, with the older group having significantly more primary osteoarthritis (78% vs. 51%), while the younger group had significantly more patients with a history of shoulder instability (48% vs. 12%), prior ipsilateral shoulder surgery of any type (74% vs. 34%), and prior ipsilateral shoulder stabilization (31% vs. 5%). In the resultant logistic regression model, a history of shoulder instability (OR 5.0) and a history of any prior ipsilateral shoulder surgery (OR 3.5) were associated with TSA prior to the age of 50 years old.
From the foregoing, it is evident that the shoulder pathoanatomy of young patients having shoulder arthroplasty is different from that of older patients - a fact that may contribute to inferior results in these individuals after shoulder joint replacement. Patient charateristics, such as higher activity levels, higher expectations, and relationships of the shoulder problem to work are also likely to contribute to the increased revision rate.

As pointed out in a prior post, the reported outcomes of shoulder arthroplasty in patients under the age of fifty years are worse than those in patients over fifty. While a number of factors, such as differences in activity level, patient longevity, and differences in expectations, have been proposed as the reason for this difference, the authors of Comparison of Patients Undergoing Primary Shoulder Arthroplasty Before and After the Age of Fifty explored the possibility that patients under fifty years of age had differences in their pre-arthroplasty self-assessed comfort and function, sex distribution, and specific type of arthritis in comparison to their more senior counterparts. Patients under the age of fifty years were not more likely than those over fifty to be female or to have a lower prearthroplasty self-assessed comfort and function score. However, they did have more complex pathological conditions, such as capsulorrhaphy arthropathy (arthritis after surgery for instability), rheumatoid arthritis, and posttraumatic arthritis. Only 21% of the younger patients had primary degenerative joint disease, whereas 66% of the older patients had that diagnosis.


They suggested that the pathoanatomy in these younger patients can complicate the surgery, the rehabilitation and the outcome of the shoulder arthroplasty. The preoperative diagnosis may have at least as much influence on the outcome of the procedure as does the age of the patient.
Recently, the authors of A History of Shoulder Instability is More Common in Young Patients Undergoing Total Shoulder Arthroplasty sought to evaluate whether a history of shoulder instability was more common in patients under 50 years old undergoing TSA. They identified 489 patients undergoing primary TSA within the Military Health System.
Patients under 50 years old were matched 1:2 with patients 50 years and older based on sex, race, and military status; the final study population comprised 240 patients.
The groups differed significantly in type of shoulder arthritis, with the older group having significantly more primary osteoarthritis (78% vs. 51%), while the younger group had significantly more patients with a history of shoulder instability (48% vs. 12%), prior ipsilateral shoulder surgery of any type (74% vs. 34%), and prior ipsilateral shoulder stabilization (31% vs. 5%). In the resultant logistic regression model, a history of shoulder instability (OR 5.0) and a history of any prior ipsilateral shoulder surgery (OR 3.5) were associated with TSA prior to the age of 50 years old.
From the foregoing, it is evident that the shoulder pathoanatomy of young patients having shoulder arthroplasty is different from that of older patients - a fact that may contribute to inferior results in these individuals after shoulder joint replacement. Patient charateristics, such as higher activity levels, higher expectations, and relationships of the shoulder problem to work are also likely to contribute to the increased revision rate.
All of these factors need to be considered in discussions with the patient prior to electing to proceed with shoulder arthroplasty as well as determining the type of arthroplasty to be used.
You can support cutting edge shoulder research that is leading to better care for patients with shoulder problems, click on this link.
Follow on twitter: https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link).
Shoulder rehabilitation exercises (see this link).
You can support cutting edge shoulder research that is leading to better care for patients with shoulder problems, click on this link.
Follow on twitter: https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link).
Shoulder rehabilitation exercises (see this link).