


After 25 years of being unable to throw overhand, she’s now back at it.

While anatomic total shoulder arthroplasty (aTSA) is a reliable treatment for osteoarthritis with an intact rotator cuff, it is not effective in managing CTA because the stabilizing effect of the rotator cuff is lacking. If CTA is treated with an aTSA, the prosthetic glenoid component is at risk for rocking horse loosening.


Refractory and disabling CTA can be managed by reverse total shoulder arthroplasty (RTSA), especially in cases of CTA having instability or inability to actively raise the arm (pseudoparalysis).

However in cases of CTA, RTSA is associated with increased risk of major complications, such as baseplate failure and acromial/scapular spine stress fracture, especially in cases where the bone is soft.


CTA-hemiarthroplasty(CTA-H) uses a humeral component with an extended humeral articular surface selected to fit the acetabularized coracoacromial arch and glenoid. It broadly distributes the load and provides a stable center of rotation for the action of the deltoid.

CTA-H is a safe, effective and durable treatment for cuff tear arthropathy in shoulders with preoperative active elevation above the horizontal. CTA-H does not carry the risks of baseplate failure, acromial/scapular spine stress fracture, dislocation, or restricted internal rotation that are associated with a reverse total shoulder.

or anterosuperior escape.



Pathophysiology
In the normal shoulder, the humeral head is centered in the glenoid throughout the joint’s range of motion by two mechanisms. The first is concavity compression in which normal cuff muscles compress the head into the glenoid concavity.

When the rotator cuff is deficient, the unopposed superiorly directed force of the deltoid muscle causes upward instability of the humeral head.

The second is the stabilizing articulation of the rotator-cuff covered humeral head with the coracoacromial arch.

When the coracoacromial arch is deficient, the upward directed deltoid force can cause antero-superior instability of the humeral head. Subscapularis deficiency may contribute further to anterior instability.

Eccentric contact of the humeral head in the glenoid and unphysiological contact of the uncovered humeral head with the coracoacromial arch can cause wear of the humeral articular cartilage leading to rotator cuff tear arthropathy.

Erosion of the superior glenoid leads to loss of the stabilizing effect of the superior glenoid concavity.

Advanced rotator cuff tear arthropathy may demonstrate loss of the prominence of the greater tuberosity (“femoralization” of the proximal humerus) and a hip-like concavity that includes the sculpted undersurface of the acromion, the coracoacromial ligament, and upper glenoid (“acetabularization” ).


The resulting ball and socket pathoanatomy invites a hemiarthroplasty in which the rough surface of the arthritic humeral head is replaced by a smooth prosthesis that fits in and is stabilized by the acetabularized concavity.

History
Cuff tear arthropathy is a degenerative condition, usually presenting as the progressive onset of pain and weakness of the shoulder. Occasionally, an injury or awkward movement can lead to an abrupt exacerbation of symptoms. Patients often give a history of prior rotator cuff surgery. It is worthwhile inquiring about symptoms that may suggest cervical spine involvement, such as night pain, radiating pain down the arm below the elbow, weakness and numbness of the hand, and pain on turning the head to the affected side.
The history should also include a pre-treatment measure of patient reported comfort and function, such as the Simple Shoulder Test. In contrast to some other outcome measures which generate a single numerical “score”, the SST documents the severity of the condition in terms of its impact on twelve individual shoulder functions. A pre-treatment SST documents the clinical severity of the CTA and serves as a baseline for measuring the effectiveness of treatment.










Treatment
Nonoperative management
Shoulder arthroplasty for the treatment of cuff tear arthropathy is an elective procedure. Thus, the patient has the opportunity to try to improve their comfort and function with non-operative management; there is no rush to the operating room. Cuff tear athropathy is a condition presenting with stiffness and weakness, which may respond to non operative management. Supervised physical therapy and home exercises can be helpful in two scenarios. In the case of the stiff shoulder – that is one that demonstrates a major loss of passive movement – the surgeon cannot determine the presence of pseudo paralysis. A trial of flexibility exercises may not only improve comfort and function, but also facilitate determination of the presence or absence of pseudoparalysis (see Video 1 and Video 2) For shoulders with good passive but poor active motion, a trial of simple strengthening exercises may mitigate apparent pseudo paralysis (see Video 3) and substantially improve the patients comfort and function.
Reverse total shoulder arthroplasty
The diagnosis of cuff tear arthropathy often leads to consideration of a reverse total shoulder (RTSA). The RTSA dramatically alters the anatomy, the mechanics, and the force distribution of the shoulder, placing non-physiologic loads on the bone of the glenoid, scapular spine and acromion. The outcomes for RTSA performed for CTA are inferior to those realized when the procedure is performed for osteoarthritis with an intact cuff. The constraint of the RTSA articulation can limit the functional range of internal rotation, compromising the ability to fasten a bra, tuck in a shirt behind, and carry out personal hygiene. Patients with CTA are at greater risk for disabling acromial and scapular spine fractures as well as glenoid baseplate failure. Dislocation, infection and periprosthetic fractures are important complications of RTSA. Instability may result from insufficient compression of the glenosphere into the humeral cup. Distalization of the humerus creates a “dead space” that may increase the risk of infection. Risk factors for complications after RTSA include inflammatory arthritis, female sex, osteoporosis, prior surgery, and cuff deficiency, each of which is more common in patients with cuff tear arthropathy.
Not uncommonly in cases of cuff tear arthropathy, the superior glenoid is eroded.

Revision of a failed reverse total shoulder is usually complicated and often unsatisfactory.
In comparison to reverse total shoulder arthroplasty, CTA hemiarthroplasty is a conservative procedure that achieves stability by replacing the arthritic humeral head with a prosthetic ball that fits within the deep socket provided by the acetabularized coracoacromial arch and upper glenoid. It preserves glenoid bone stock, not requiring reshaping of the glenoid or the insertion of screws in it. Instead of changing the loading of the acromion and scapular spine, the CTA head articulates with and supports the arch. The humeral head articular surface has a lateral extension that broadens the contact area between the humerus and the coracoacromial arch and avoids unwanted contact between the tuberosity and the acromion. The CTA hemiarthroplasty does not limit functional internal rotation.


When the indications for a CTA-H are respected, dislocation, acromial/spine fractures, and loss of fixation are infrequent, even in shoulders with compromised bone quality. Because of the lack of constraint, functional limitation of internal rotation is uncommon. The lack of dead space reduces the risk of infection.
In contrast to the difficulties in managing a failed RTSA, should a CTA-H fail to achieve the desired result, revision to a RTSA is relatively straightforward because of the preservation of humeral and glenoid bone stock.
Surgical technique
· Patient preparation and positioning

· Surgical approach




· Sizing and preparation of proximal humerus



· Stem and head selection

Recognizing that the bone of patients with CTA is often weak, care is taken to avoid any endosteal reaming that could create a diaphyseal stress riser at the distal tip of the implant. Because a smaller filling ratio is desired to minimize stress shielding and reduce the risk of fracture, the humeral body implant is slightly undersized with the plan to stabilize the final component with impaction grafting.
A trial head matching the curvature of the resected anatomic head is placed on the trial body allowing the surgeon to check range of motion and stability. The trial component should tension the deltoid so that it rests in 30 degrees of abduction, and springs back to that position when the arm is passively adducted and released (the “spring test”). If the shoulder lacks the desired spring, a thicker head can be trialed. The shoulder should have 150 degrees of flexion and 60 degrees of internal rotation with the arm in 90 degrees of abduction.


· Impaction grafting
Using bone from the resected humeral head, the canal is impaction-autografted using a trial body component until a snug, stable fit is achieved.

Preparation for subscapularis repair and possible biceps tenodesis


· Prosthesis insertion


· Subscapularis repair


Post operative care
For the first six weeks the patient focuses on passive flexion in the supine position (see Video) and using a pulley (see Video) avoiding external rotation beyond zero degrees and avoiding active elevation of the arm. The patient is cautioned to avoid pushing off of bed or chair with surgical shoulder.
For the second six weeks the active supine press (see Video) is added, starting with two hands together, then with two hands apart, then with one hand alone, then with progressive inclination. Once twenty repetitions can be comfortably carried out at one level, the patient can advance to the next level.
At twelve weeks the patient can gradually return to desired activities without restriction, taking small steps and keeping his/her shoulder comfortable.
Outcomes
A review of the published literature on the outcomes of anatomic shoulder arthroplasty for CTA has informed our current indications and surgical technique.Neer et al recommended treating cuff tear arthropathy with anatomic total shoulder arthroplasty combined with attempting rotator cuff repair. Barrett et al and Franklin et al demonstrated that in the presence of rotator cuff deficiency, the glenoid components of total shoulders were at risk for rocking-horse loosening. Pollock et al found that hemiarthroplasty combined with attempting rotator cuff repair made approximation of the cuff easier by avoiding the thickness of the glenoid component. Out of concern for the high rate of failure of cuff repair in cases of CTA, Arntz et al pioneered the novel approach of using a standard hemiarthroplasty component inserted without attempting cuff repair, allowing the humeral component to articulate with the carefully preserved coracoacromial arch and using a head thickness that put the deltoid and residual cuff under appropriate, but not undue tension. Applying this same surgical philosophy, Arntz et al and Williams et al offered hemiarthroplasty to patients with CTA without attempting cuff repair, emphasizing the importance of an intact coracoacromial arch. Most patients were satisfied, had relief of pain and improved active flexion by more than 50 degrees. No patients were revised because of instability, acromial fractures, or glenoid component failure. Field et al, Zuckerman et al, and Sanchez-Sotelo et al emphasized the importance of the integrity of the coracoacromial arch, noting that patients with prior acromioplasty and release of the coracohumeral ligament experienced anterosuperior instability and unsatisfactory results. Goldberg et al pointed out that CTA patients with active preoperative elevation greater than 90 degrees had good functional results from hemiarthroplasty.
Visotsky et al were the first to report on the management of cuff tear arthropathy with an extended humeral head hemiarthroplasty. The rationale of this implant was to provide (1) increased articular surface contact between the humerus and the coracoacromial arch, (2) coverage of the exposed greater tuberosity with a smooth joint surface, avoiding unwanted contact between the tuberosity and the acromion, and (3) increased stability from compression of the humeral convexity into the coracoacromial/upper glenoid concavity. Using this implant, they reported substantial improvement in shoulder comfort and function for patients having CTA of Seebauer Types IA, IB, and IIA. For those with anterosuperior escape (Seebauer type IIB) they recommended reverse total shoulder arthroplasty. Similar indications and outcomes for the extended head hemiarthroplasty were reported by Arnold et al, Firestone et al, and Filho et al.

{kind=link}
Matsen et al (Clinical effectiveness and safety of the extended humeral head arthroplasty for selected patients with rotator cuff tear arthropathy), Chawla al (Drivers of inpatient hospitalization costs, joint-specific patient-reported outcomes, and health-related quality of life in shoulder arthroplasty for cuff tear arthropathy), Stenson et al (Managing rotator cuff tear arthropathy: a role for cuff tear arthropathy hemiarthroplasty as well as reverse total shoulder arthroplasty) pointed to the clinical effectiveness and safety of the extended humeral head arthroplasty in patients having rotator cuff tear arthropathy with preoperative active elevation above the horizontal. They specifically noted the improvement in patient self-assessed shoulder comfort and function in the absence of complications such as dislocation, glenoid component failure and acromial/scapular spine stress fracture. These studies along with that of Coe et al (The cost-effectiveness of reverse total shoulder arthroplasty compared with hemiarthroplasty for rotator cuff tear arthropathy) suggest that because of the greater cost and complication rate of a reverse total shoulder, the CTA hemiarthroplasty with an extended humeral articular surface is a more cost-effective approach to cuff tear arthropathy in patients without pseudoparalysis or instability. This may be particularly the case for patients with reduced bone density (making them more prone to acromial/spine fractures and baseplate failure) and those wishing to avoid restriction of reach up the back or cross body. We recently evaluated prospectively enrolled patients having cuff tear arthropathy with preoperative active elevation above the horizontal who elected to undergo CTA hemiarthroplasty after a discussion of the alternative of reverse total shoulder arthroplasty. The procedure was performed through a standard deltopectoral incision, taking care to preserve the coracoacromial arch as shown in this Video. Assisted flexion was started immediately after surgery, transitioning to progressive flexion strengthening at six weeks. The patients were encouraged to return to their activities as tolerated without limitation including heavy lifting and impact activities. Sixty-seven patients had clinical follow-up at two years and were longitudinally followed as long as 11 years after the procedure using the Simple Shoulder Test (SST) to document their self-assessed comfort and function.

This is the largest series of clinical outcomes for patients having cuff tear arthropathy with preoperative active elevation who were managed with extended head humeral hemiarthroplasty (soon to be published). Fifty-five percent of the patients were male, the average age at surgery was 70±10 years.
Pre-operatively, the 67 patients had a mean SST score of 3 (IQR, 1-5). Only 15% could sleep comfortably, 19% could wash the back of the opposite shoulder, 33% could reach behind their back to tuck in a shirt, and 40% could place a coin on a shelf at shoulder level.
At two years post-operatively, the 67 patients had a mean SST score of 8 (IQR, 5-10). 76% could sleep comfortably, 61% could wash the back of the opposite shoulder, 81% could reach behind their back to tuck in a shirt, and 87% could place a coin on a shelf at shoulder level.
At minimum five years post-operatively (n=26), the mean SST score remained 8 (IQR, 7-10).
At minimum ten years post-operatively (n=9): the mean SST score remained 8 (IQR, 6-10). The longest follow-up was 13-year follow-up in a patient with an SST score of 10.
Reoperation was performed in 3 patients (4.5%): one had a debridement for infection; one was converted to a reverse total shoulder after developing pseudoparalysis from a fall after five years of good comfort and function; and one was converted to a reverse total shoulder one year after surgery because of anterosuperior escape.
Complications: there were no cases of acromial or scapular spine fracture, dislocation, or scapular notching.
The outcome story of CTA-hemi is told not only by numbers, but also by the stories of individual patients who wished to avoid the risks and limitations of a reverse total shoulder and who had durable recovery of comfort and function. The figures below demonstrate six typical cases.
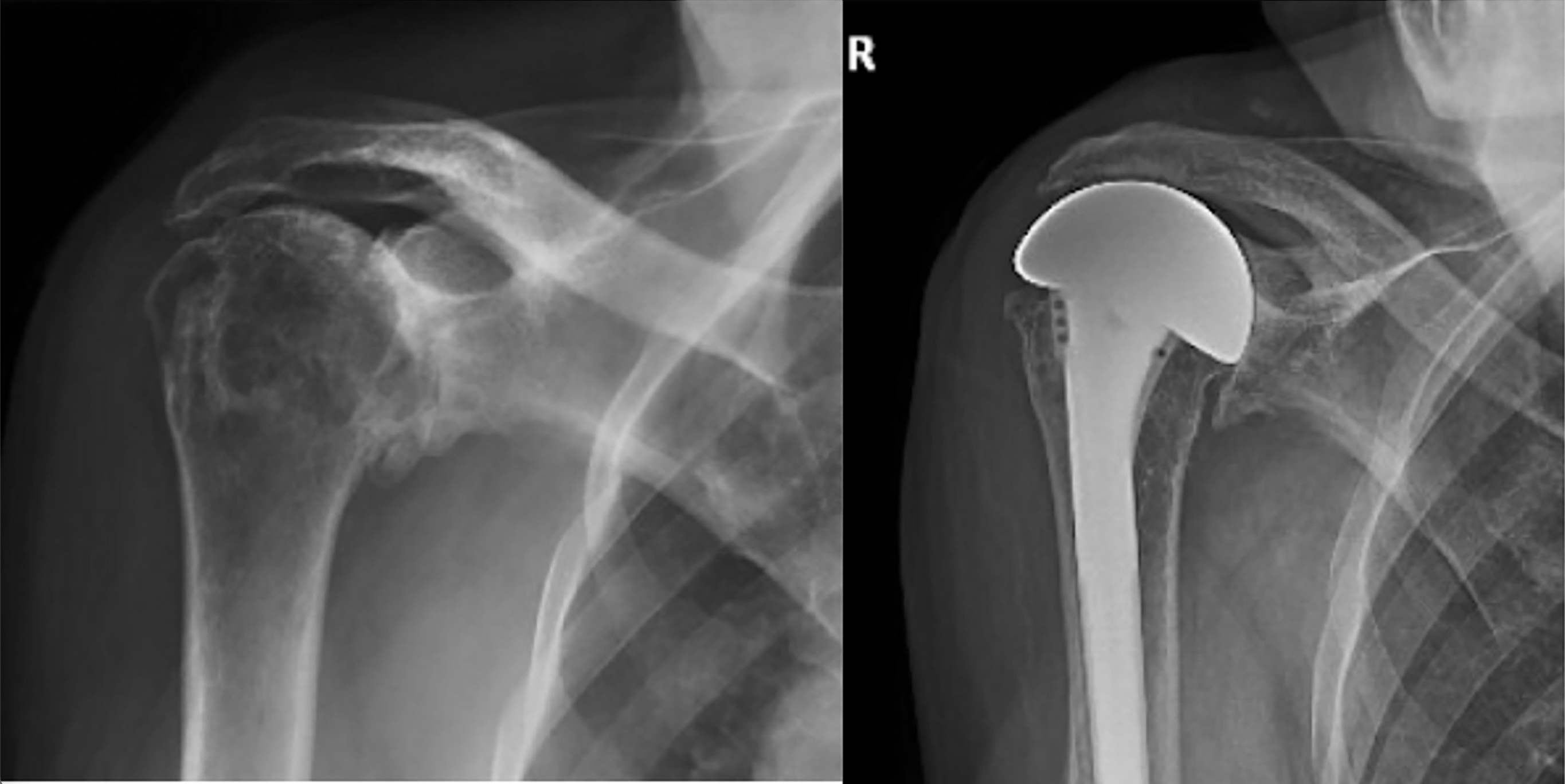
Case 1: A woman rancher in her early 60’s with arthritis, irreparable subscapularis, supraspinatus, and upper infraspinatus tears, and retained active elevation above the horizontal. Her preoperative and postoperative x-rays are shown here.


Case 2: An active woman in her 60’s with cuff tear arthropathy of the left shoulder after two failed rotator cuff repairs was referred for consideration of a reverse total shoulder arthroplasty. She has seronegative rheumatoid arthritis treated with prednisone, Avara, and methotrexate. Her preoperative x-ray shows diminished bone density, placing her at increased risk for acromial/spine fracture with a reverse total shoulder.

At 4.5 years after her CTA-H procedure she reported that she had returned to her desired activities. Her shoulder was comfortable and able to perform 10 of the 12 functions of the Simple Shoulder Test, including the ability sleep on that side, to internally rotate the arm to tuck in her shirt behind her, to wash the back of the opposite shoulder, to lift eight pounds to shoulder level, as well as to toss and throw a ball. Her SANE score was 100. She could actively elevate her arm to 140 degrees.

Case 3: X-rays shown below for an active muscular man in his early 60’s presented with a painful right shoulder after several failed attempts a rotator cuff repair. He had a stable shoulder and retained active elevation despite having irreparable subscapularis, supraspinatus, and infraspinatus tendon tears.

At one year after surgery, he returned with a comfortable shoulder with full active motion and progressively improving strength. Despite his subscapularis deficiency, he reported no problems with instability.

Case 4: An active man in his 70’s presented with pain and loss of function in his right shoulder. Despite having irreparable supraspinatus and infraspinatus tears and a torn subscapularis, he had active elevation above 90 degrees. At surgery his subscapularis was reconstructable. His preoperative and postoperative x-rays are shown here.

At three years after surgery, he returned for routine follow-up with a comfortable functional shoulder.

Case 5: A 60-year-old lady with rheumatoid arthritis and osteoporosis. presented with pain and loss of function in the left shoulder. Her subscapularis, supraspinatus, and infraspinatus were irreparably torn. Her preoperative and 12-year postoperative x-rays are shown here.

At 12 years after surgery her shoulder was comfortable and functional. She had no issues with fracture of the acromion or scapular spine even though she had several major risk factors.

Case 6: A 71-year-old man presented with cuff tear arthropathy and retained active elevation. His preoperative and 11-year postoperative films are shown here.
At eleven years after surgery, his shoulder was comfortable and functional.

Case 7: A 77-year-old retired physician, active rancher presented with pain and loss of function of the left shoulder after prior rotator cuff surgery. His preoperative and 11-year postoperative x-rays are shown here.

Now at the age of 88 he is still active on his ranch without shoulder limitation despite taking occasional falls as he traverses the woods on his property.

In conclusion, CTA-hemiarthroplasty is a strong consideration for patients with cuff tear arthropathy and retained active elevation.
You can support cutting edge shoulder research that is leading to better care for patients with shoulder problems, click on this link
Follow on twitter/X: https://x.com/RickMatsen
Follow on facebook: https://www.facebook.com/shoulder.arthritis
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link).
Shoulder rehabilitation exercises (see this link).