
Patients and surgeons are interested in knowing the relationship of relative body weight to the rate of adverse events following shoulder arthroplasty. Are patients who have higher BMI (click here to see how to calculate yours) at greater risk?
The authors of High and Low Body Mass Index Increases the Risk of Short-Term Postoperative Complications Following Total Shoulder Arthroplasty. reviewed the 30-day adverse events for 22,132 patients having total shoulder arthroplasty with known preoperative BMI's.
Interestingly, patients with BMI > 30 kg/meter squared did not have significantly different rates of adverse events than those with BMI < 30 kg/meter squared. Case closed, right?
No.
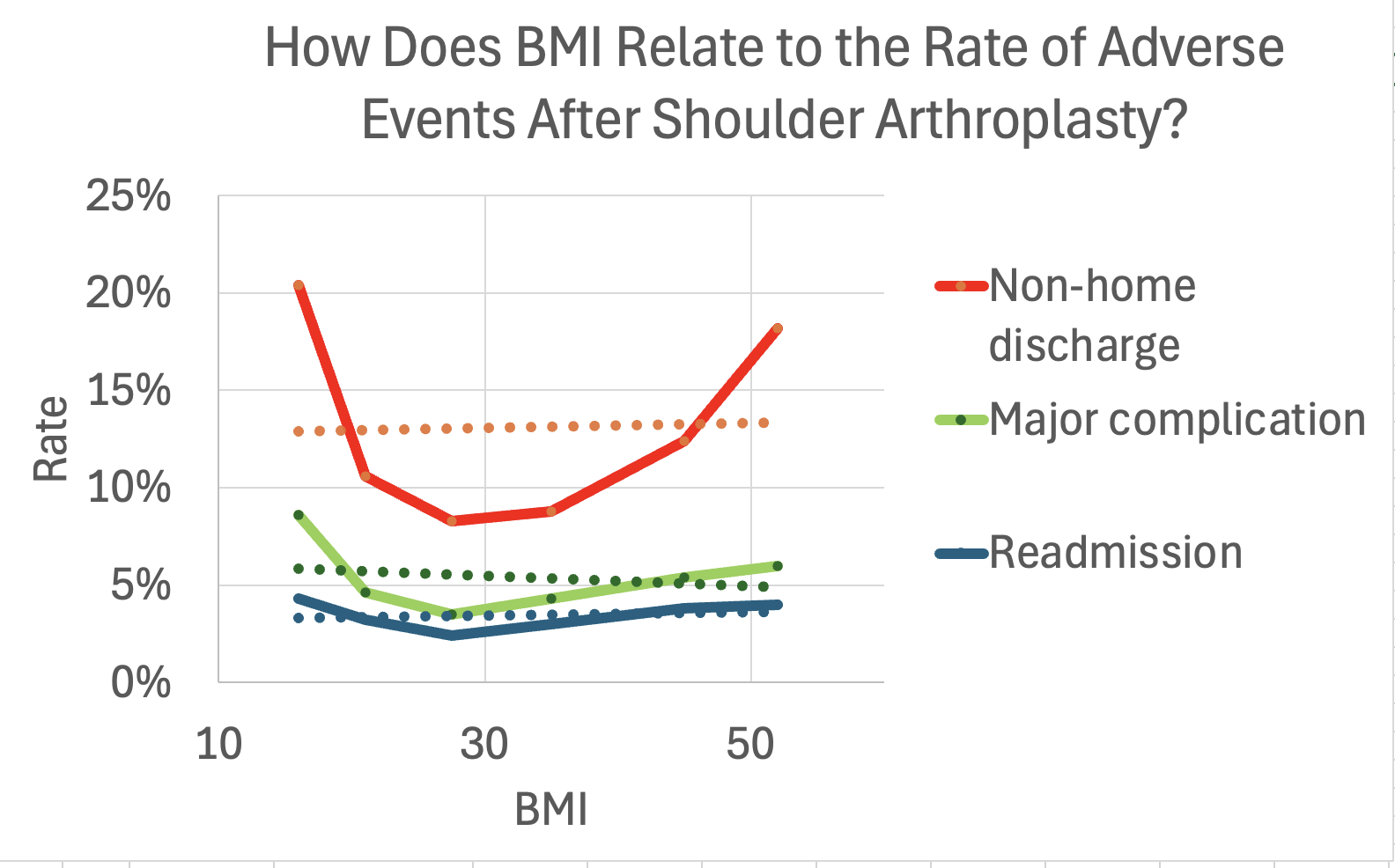
When they divided the patients into five groups: BMI <18.5, BMI 18.5-24.9, BMI 30-39.9, BMI 40-49.9, and BMI ≥ 50 a different story unfolded as seen in the scatter plot below, which shows that the overweight (BMI 30-39.9), but not obese, patients had the lowest rate of adverse events. Furthermore, the real uptick in adverse events was found only for the BMI <18.5 and the BMI ≥ 40 patients.

There is another lesson here. If we (as we often do) blindly look for a relationship between one thing and another using linear regression, we would completely miss the important relationship shown above. Note in the graph below, the linear regression trend lines are all flat as a pancake, with "no significant relationship" (sic).

Comments welcome at shoulderarthritis@uw.edu
You can support cutting edge shoulder research that is leading to better care for patients with shoulder problems, click on this link
Follow on twitter/X: https://x.com/RickMatsen
Follow on facebook: https://www.facebook.com/shoulder.arthritis
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link).
Shoulder rehabilitation exercises (see this link).
You can support cutting edge shoulder research that is leading to better care for patients with shoulder problems, click on this link
Follow on twitter/X: https://x.com/RickMatsen
Follow on facebook: https://www.facebook.com/shoulder.arthritis
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link).
Shoulder rehabilitation exercises (see this link).



