
The rotator cuff has two main functions in the shoulder: (1) it stabilizes the humeral head in the glenoid socket and (2) it works with the deltoid and other shoulder muscles to help provide the strength necessary for the shoulder to do its work.
In this video, one can see how the supraspinatus tendon, the most commonly injured tendon of the rotator cuff, normally passes smoothly below the coracoacromial arch as the arm is lifted from the side in this cadaver demonstration.
In this video, one can see how the supraspinatus tendon, the most commonly injured tendon of the rotator cuff, normally passes smoothly below the coracoacromial arch as the arm is lifted from the side in this cadaver demonstration.
For a short cut to an overview of the cuff and the spectrum of rotator cuff disease, see this page and the gallery on its right.
You may also like to see our recent review of rotator cuff failure from the New England Journal of Medicine.
---
We'll take a step back and consider some of the principles of shoulder strength in depth.
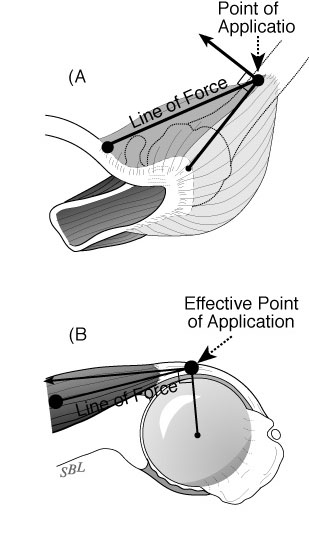
When a muscle contracts, it approximates its effective origin and insertion with a force limited by its physiological cross sectional area. Muscles that have large cross sections, like the deltoid, can provide a larger maximal force than a muscle with a small cross section like the subclavius. The contractile elements within a muscle are connected to tendon fibers that connect to the bony origin and insertion. The tendon insertion is structured so that there is a smooth mechanical transition from flexible tendon to stiff bone.

This smooth transition enables the insertion to manage the repeated bending loads to which it is subject.

When the tissues providing this smooth transition degenerate they become stiff and weak so that the tendon insertion becomes increasingly vulnerable to failure.


The effective points of attachment depend on the position of the arm and are not necessarily the anatomic insertions .

Throughout this discussion, the lever arms have been described as the distance between the point of action of the muscle force and the center of rotation. In order for torques to be realized, the humerus must rotate around a stable center. This is why we have placed such emphasis on the mechanisms for centering of the head in the section on Stability. Without this precise centering, the effectiveness of the muscle contractions would be lost.
Muscles are also characterized by their excursion – the change in length over which they can provide force. In order to be effective throughout a range of motion, the centimeters of excursion of a muscle must match the product of the muscle’s lever arm in centimeters and the range of motion in degrees divided by the number of degrees in a radian.

So, while longer lever arms result in more torque per unit muscle force, they also require greater muscle excursion.


Muscles that have been chronically detached, as in long standing cuff tears, tend to lose their excursion. Even if they are reattached, the length over which they can exert an effective force is often diminished.
A special feature of the shoulder is that the powerful thoracoscapular muscles can position the entire glenohumeral joint along with the deltoid and the rotator cuff through a range of approximately 40 degrees of adduction/abduction


One of the relatively unexplored facets of active shoulder strength is the requirement for muscular balance. In the knee, the muscles generate torques about a relatively fixed axis: that of flexion-extension. If the quadriceps pull is a bit off-center, the knee still extends. In the shoulder, no such fixed axis exists. In a specified position, each muscle creates a unique set of rotational moments. Imagine a rope attached to a sphere. The motion resulting from pulling on the rope depends on the orientation of the sphere as well as the direction of pull on the rope. If some of the resulting motion were undesired, it would need to be cancelled out by attaching another rope and pulling on it to resist the unwanted motion. So, for example, the anterior deltoid exerts moments in forward elevation, internal rotation, and cross-body movement.

If elevation without cross body movement is desired, the posterior deltoid must negate the cross body moment of the anterior deltoid.
Similarly, if elevation without rotation is desired, the cross-body and internal rotation moments of this muscle must be resisted by other muscles (such as the posterior deltoid and infraspinatus). These balancing activities take place at an additional energy cost. However, if the infraspinatus function is lacking, it is difficult to flex the arm without internal rotation.

{kind=link}
--
How you can support research in shoulder surgery Click on this link.
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link).
Shoulder rehabilitation exercises (see this link).