
Because shoulder arthroplasty is performed through a transection of the subscapularis attachment to the humerus - either a tenotomy, an incision at the bone tendon junction or a lesser tuberosity osteotomy. Regardless of the method of detachment, careful repair and postoperative protection of the repair are necessary to prevent failure of the reattachment (see this link). If the reattachment fails, something more than a simple reattachment is often necessary.
Here's an illustrative case: a 77 year old male had a total shoulder arthroplasty in 2012. He did well initially after his surgery and was quite diligent about following his rehab protocol. Unfortunately at 3 months post operatively he was reaching for an object he felt a twinge in his shoulder and afterwards it did not feel quite right. On exam he had 80 degrees of passive external rotation with weakness in internal rotation concerning for a subscapularis tear. His only complaint was the tendency of his shoulder to slip anteriorly with external rotation and extension. Otherwise his shoulder was comfortable and functional. An axillary x-ray suggested anterior subluxation of the humeral head on the glenoid.

Of note he did have a history of previous rotator cuff tears in the contralateral right shoulder with two attempted repairs several years prior to his arthroplasty procedure. He was also taking chronic steroids for adrenal insufficiency.
Our approach to the evaluation of management of subscapularis deficiency has been described (see this link).
In this case surgery had to be delayed due to pressing medical issues for over a year.
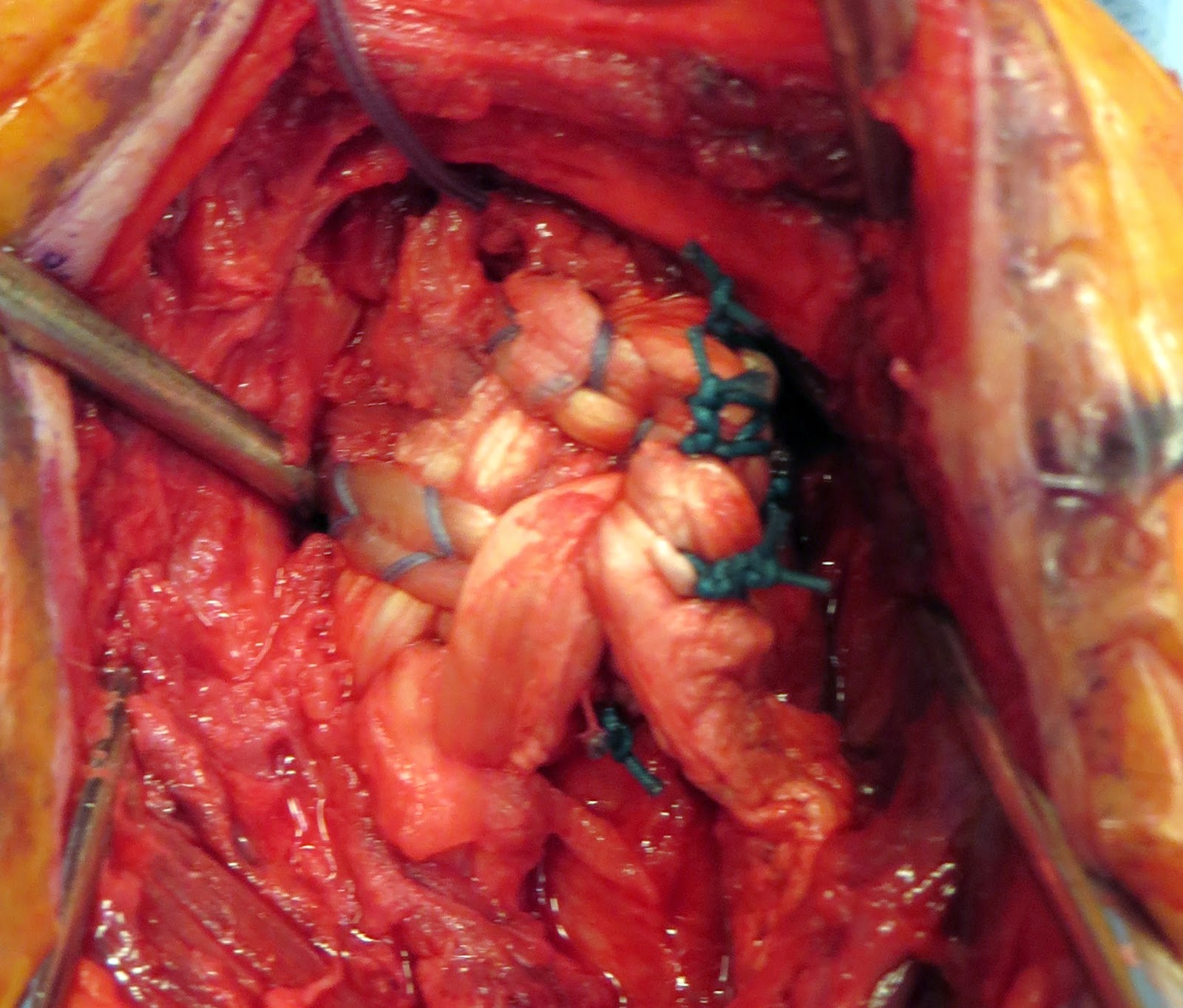
At the time of surgery his subscapularis tendon was torn with the bulk of the tendon retracted and scarred underneath the conjoined tendon. Great care was taken to release these adhesions and mobilize the subscapularis due to the close proximity of neurovascular structures and altered surgical field with scar tissue.
After the subscpularis was mobilized, a burr was used to create a transosseus tunnel in the bicipital groove separated by a 2cm bone bridge. The allograft was passed through this tunnel and then each end was woven through the native subscapularis tendon medially. After securing the native subscapularis to the lesser tuberosity with sutures, the allograft was looped over itself in a figure of 8 and secured laterally with suture. The quality of the repair afterwards was excellent with 0 degrees of external rotation and a firm endpoint.


His postoperative film shows centering of the humeral head on the glenoid.

He will be protected in internal rotation for 6 weeks.
This post prepared with the collaboration of Robert Lucas, M.D.
Consultation for those who live a distance away from Seattle.
Click here to see the new Rotator Cuff Book
To see the topics covered in this Blog, click here
Use the "Search" box to the right to find other topics of interest to you.
You may be interested in some of our most visited web pages including:shoulder arthritis, total shoulder, ream and run, reverse total shoulder, CTA arthroplasty, and rotator cuff surgery as well as the 'ream and run essentials'
You may be interested in some of our most visited web pages including:shoulder arthritis, total shoulder, ream and run, reverse total shoulder, CTA arthroplasty, and rotator cuff surgery as well as the 'ream and run essentials'