Clinical outcomes and temporal changes in the range of motion following superior capsular reconstruction for irreparable rotator cuff tears: comparison based on the Hamada classification, presence or absence of shoulder pseudoparalysis, and status of the subscapularis tendon
These authors report their outcomes for 54 consecutive patients with irreparable rotator cuff tears or pseudoparalysis (PPS) who underwent superior capsular reconstruction (SCR) using autologous tensor fascia lata with an average graft thickness of 8.3 mm.
The inclusion criterion for SCR was an irreparable rotator cuff tear or PPS with failed conservative treatment, supervised by physiotherapists, for >6 months. In all patients, the Hamada classification was grade 2 in 11 patients and grade 3 in 43 patients.

Included shoulders had a Goutallier grade 3 or higher fatty infiltration of the tendon with the tendon retracted to the glenoid level as evaluated on magnetic resonance imaging and torn tendons that could not reach the original footprint after the release of soft tissues at the time of surgery.
Pseudoparalysis (PPS) was defined as
(1) moderate PPS (n=16), no shoulder stiffness, active shoulder elevation (both flexion and abduction) ≤ 90 degrees , and the ability of the patient to maintain ≥ 90 degrees of elevation once the shoulder was passively elevated;
(2) severe PPS (n=16), comprising no shoulder stiffness, active shoulder elevation ≤ 90 degrees, and the inability of the patient to maintain ≥ 90 degrees of elevation once the shoulder was elevated passively; and
(3) non-PPS (n=22), comprising no shoulder stiffness and active shoulder elevation > 90 degrees.
Lidocaine was routinely injected into the subacromial space preoperatively; patients whose ROM improved were considered to have a painful loss of elevation and were not considered as patients with PPS.
Patients who could not elevate their shoulders even in the supine position were considered to have deltoid insufficiency and were excluded from this study.
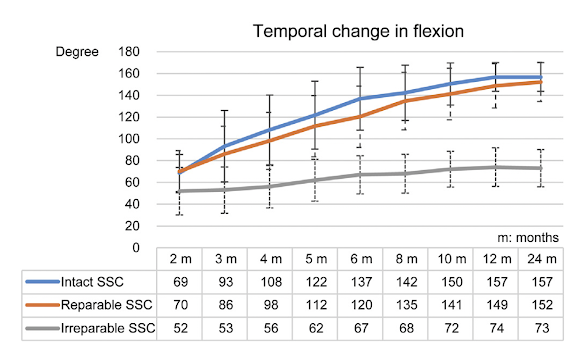
The 32 PPS patients were divided into 3 groups: intact subscapularis (SSC) (11 patients), repairable SSC (16 patients), and irreparable SSC (5 patients).
They found no significant differences in postoperative ASES scores and shoulder range of motion between the Hamada grade 2 and grade 3 groups or between the non-PPS, moderate PPS, and severe PPS groups. PPS patients required a longer duration to achieve shoulder elevation > 130 degrees; nevertheless, the authors found no significant differences in final outcomes between the non-PPS and PPS groups.

However, significant differences in postoperative ASES scores were observed between the intact SSC (final ASES = 91) and irreparable SSC groups (final ASES = 56) and between the repairable SSC (final ASES = 92) and irreparable SSC groups (final ASES = 56). There were significant differences in postoperative shoulder elevation (see graph below). The repairable SSC tear group tended to take longer to achieve improvement in shoulder elevation than the intact SSC group, although the final outcomes between the 2 groups did not show a significant difference.
The patients noted to have anatomic failure of the SCR had excellent shoulder function and no or minimal pain as did patients with partial failure of the subscapularis repair.
The authors concluded that the status of the subscapularis, rather than the Hamada grade or the presence or absence of PPS, influenced the clinical outcomes in this series of SCRs.
Comment: This study demonstrates the importance of the subscapularis integrity in the functional outcomes of reconstruction for irreparable rotator cuff tears. It also demonstrates the potential for reversing pseudoparalysis using superior capsular reconstruction with autologous tensor fascia and the timeframe for recovery.
The application of superior capsular reconstruction, rather than reverse total shoulder, is interesting and requires further clinical investigation of indications, technique and outcomes.
Follow on twitter: https://twitter.com/shoulderarth
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Shoulder arthritis - what you need to know (see this link) Shoulder arthritis - x-ray appearance (see this link) The smooth and move for irreparable cuff tears (see this link) The total shoulder arthroplasty (see this link). The ream and run technique is shown in this link. The cuff tear arthropathy arthroplasty (see this link). The reverse total shoulder arthroplasty (see this link).
Shoulder rehabilitation exercises (see this link).
This is a non-commercial site, the purpose of which is education, consistent with "Fair Use" as defined in Title 17 of the U.S. Code.
Note that author has no financial relationships with any orthopaedic companies.







































