
Variation in the Value of Total Shoulder Arthroplasty
These authors identified 239 patients having elective primary TSA (anatomic or reverse) and calculated
value as 2-year postoperative American Shoulder and Elbow Surgeons (ASES) scores divided by hospitalization time-driven activity-based costs.
Lower value was observed in women, unmarried patients, younger patients, those with more self-reported allergies, greater BMI, lower preoperative ASES score, ASA score ≥ 3, preoperative daily opioid use, diabetes, prior ipsilateral shoulder surgery, and patients undergoing reverse rather than anatomic total shoulder.
On multivariable analysis, reverse shoulder arthroplasty was associated with decreased value compared to anatomic shoulder arthroplasty, as were prior shoulder surgery, more self-reported allergies, diabetes, and lower preoperative ASES score.
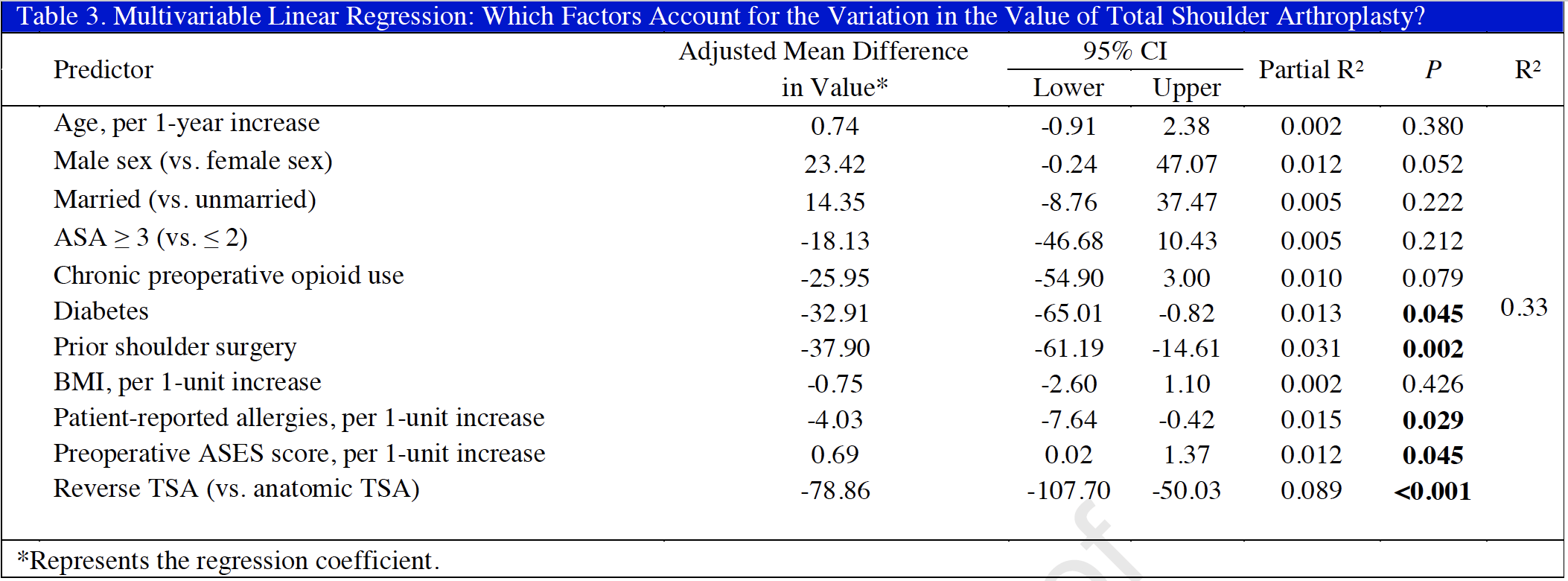
Procedure type alone accounted for 8.9% of the observed variation in value, while prior ipsilateral shoulder surgery explained 3.1% of the variation, number of self reported allergies 1.5%, diabetes 1.3%, and preoperative ASES score 1.2%.
Taken together, patient characteristics and procedure type accounted for 33% of the observed variation in value of shoulder arthroplasty, while 66% of the variation remained unexplained.
Comment: Of the variables identified as being important drivers of cost, the only one that is controlled by the surgeon is the choice between reverse and anatomic total shoulder. This is important in light of the current trend to use reverse total shoulder rather than anatomic total shoulder in the management of osteoarthritis with an intact rotator cuff.
In this study the benefit of arthroplasty was assessed by the two year postoperative ASES score. However, as expected, patients with higher preoperative ASES scores tended to have higher postoperative scores. As a result, surgeons selecting less severely involved shoulders for arthroplasty would achieve higher value. Perhaps a better measure of benefit to the patient would be the preoperative to postoperative change, or the percent of maximal possible improvement (postoperative ASES score minus preoperative ASES score divided by 100 minus the preoperative ASES score).
These authors used sophisticated methods for assessing the hospital costs. However, the total costs of an arthroplasty also included those associated with preoperative imaging, surgeons' fees, anesthesiologists' fees, and postoperative rehabilitation. The costs of an arthroplasty should also include the costs of complications, readmissions and revisions; the total value of a procedure with a 10% revision rate is likely to be less than one with a 5% revision rate.
As a specialty we need to explore better methods for assessing the value to the patient of what we attempt to do for them. This type of assessment is especially important for new technologies - do they add value for the patient over and above that of the techniques in common usage?

===
How you can support research in shoulder surgery Click on this link.
We have a new set of shoulder youtubes about the shoulder, check them out at this link.
Be sure to visit "Ream and Run - the state of the art" regarding this radically conservative approach to shoulder arthritis at this link and this link
Use the "Search" box to the right to find other topics of interest to you.