

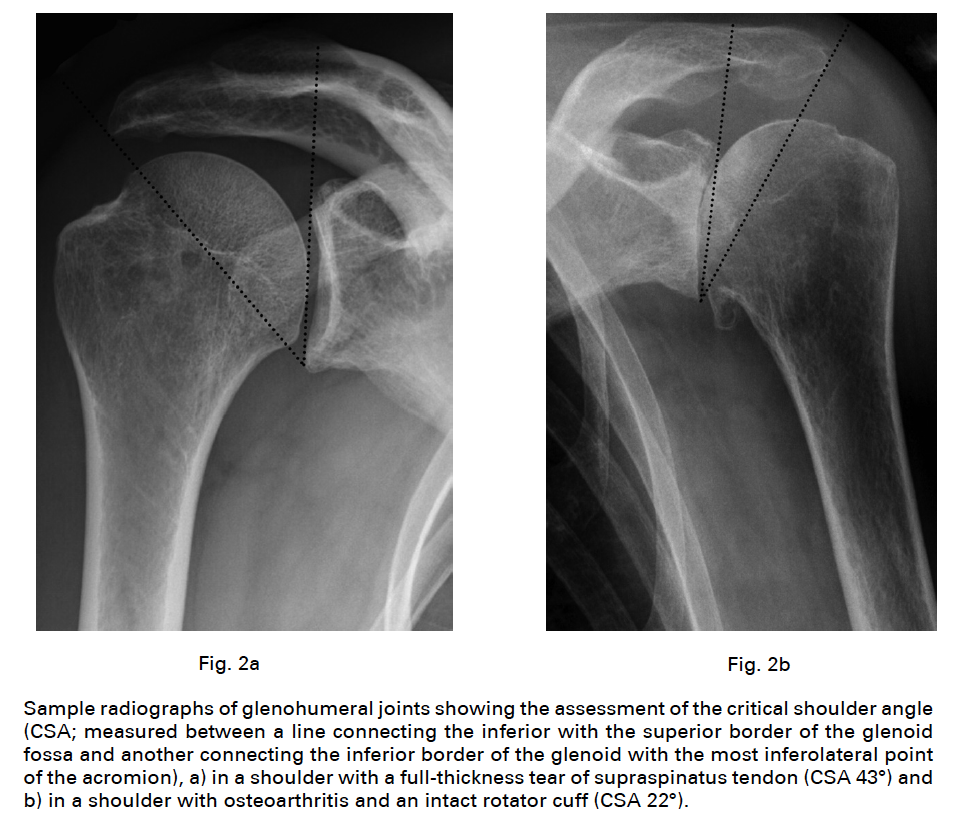
It is of note in the 2013 description of the critical shoulder angle, Is there an association between the individual anatomy of the scapula and the development of rotator cuff tears or osteoarthritis of the glenohumeral joint?, the authors hypothesised that a large acromial cover with an upwardly tilted glenoid fossa would be associated with degenerative rotator cuff tears (RCTs), and conversely, that a short acromion with an inferiorly inclined glenoid would be associated with glenohumeral osteoarthritis (OA). They found that if the CSA was < 30°: 80 shoulders (93%) were osteo-arthritic. If the CSA was between 30° and 35° 78 of these shoulders (70%) had neither cuff tears or osteoarthritis, 18 (16%) had OA and 14 (14%) had cuff tears. When the CSA was > 35°: 84 (84%) were in the RCT group and only four (4%) in the OA group.
The authors of the current article conducted a matched case-control study using a shoulder arthroplasty registry from the Kaiser-Permanente healthcare system of patients who underwent primary elective anatomic total shoulder arthroplasty (TSA) for osteoarthritis.
The cases included 78 patients that underwent revision due to glenoid component failure or rotator cuff tear. Of the 78 cases, 25 were revised due to glenoid failure, 47 were revised due to rotator cuff tear, and 6 had both indications.
Two non-revised controls were matched to each case by age, gender, body mass index, American Society of Anesthesiologists classification, surgeon who performed the index TSA, and post-TSA follow-up time.
Revised cases had a higher likelihood of a critical shoulder angle (CSA) ≥35° (odds ratio [OR]=2.41, 95% confidence interval [CI]=1.27-4.59).
A higher likelihood of CSA ≥35° was observed for those revised for glenoid loosening (OR=4.58, 95% CI=1.20-17.50) and revised for rotator cuff tear (OR= 2.41, 95% CI=1.18-4.92) compared to non-revised controls.
Every 5° increase in CSA had higher odds of overall revision (OR=1.62, 95% CI=1.18-2.21), glenoid loosening (OR=2.50, 95% CI=1.27-4.92), and rotator cuff tear (OR=1.51, 95% CI=1.07-2.14).

These authors suggest that a reverse arthroplasty might be considered in cases of primary shoulder arthritis with a CSA of 35° or greater.
Comment: This is an interesting study that brings up some interesting questions.
(1) The patients in the two groups were matched for age, gender, body mass index, and American Society of Anesthesiologists classification, surgeon and followup time, should they not have been matched for glenoid type - a factor that reflects the three-dimensional anatomy of the arthritic shoulder, that may be related to the CSA, and that has been associated with revision rate?
(2) The authors' database has enrolled 5274 TSA patients of which 78 underwent revision for glenoid component or cuff failure. That is a low revision rate of 1.4%. Is there evidence that a lower revision rate would have been achieved if a reverse total shoulder had been performed in these 78 shoulders (see the comparison of revision rates on this link)?
(3) The data in the table above show that the difference in the average CSA between the revised and non-revised shoulders was only 2 degrees; is this small difference sufficient to change the forces that might contribute to TSA failure?
(4) Over 75% (60/78) of the revised shoulders had a CSA < 35 degrees; how did the characteristics and failure modes for these shoulders compare with the 18 revised shoulders with CSA≥35?
(5) The CSA can be increased by superior glenoid inclination and by an increased length of the acromion; would it not be interesting to consider the independent effect of each of these measurements?
Follow on twitter: https://twitter.com/shoulderarth
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
How you can support research in shoulder surgery Click on this link.
Here are some videos that are of shoulder interest