
The ream and run procedure (RnR) is a glenohumeral arthroplasty considered for patients who wish to avoid the risks and activity limitations associated with a prosthetic glenoid replacement.
Here's an example of the postoperative function in a 57 year old man five years post op.




One of the major centers participating in the advancement of the ream and run procedure is the Department of Orthopaedic Surgery, Warren Alpert Medical School of Brown University, Providence, RI. Last year these surgeons published Early outcome of humeral head replacement with glenoid reaming arthroplasty (Ream and Run) for treatment of advanced glenohumeral osteoarthritis evaluating their short- and midterm outcomes for this procedure in 49 shoulders (mean age 60 years, 43 males) with minimum 2-year follow-up (mean 4.6 years). Thirteen (26.5%) had previous nonarthroplasty shoulder surgery. Most of the shoulders (61%) had type B glenoids.
After RnR, three patients underwent revision arthroplasty due to pain without obvious signs of infection at a mean of 1.9 years. One of the 3 patients had repeat RnR, with an excellent final outcome. Cultures were positive for Cutibacterium acnes, and the humerus was loose at revision. A second patient was revised to aTSA and had positive C. acnes cultures at revision. The third was revised to RSA; culture data were unavailable. No manipulations or capsular releases were performed after RnR.
After aTSA two patients underwent revision arthroplasty for glenoid loosening, at 9.2 and 14 years, and both were converted to hemiarthroplasty. At revision, cultures were positive for C. acnes for 1 patient, and negative for the other.
Comment: These two studies demonstrate that both RnR and aTSA are valuable procedures for patients with glenohumeral arthritis. In that revisions for glenoid component loosening typically occur years after aTSA, comparative studies with 10 or more years of followup will be necessary to better understand the relative advantages of the two approaches. The ream and run has now been around long enough that 10+ year followups are becoming available that show durability and applicability to complex glenoid pathologies without the need for 3D planning or augmented glenoid components.

Postoperative restrictions to protect a prosthetic glenoid component are not necessary after the ream and run procedure as shown in this video.
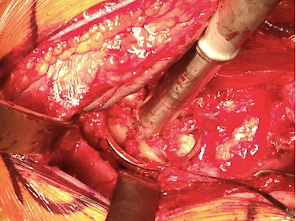
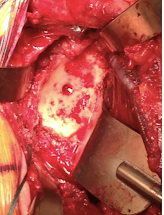
The glenoid was reamed to a diameter of curvature 4-6 mm greater than that of the selected humeral component, preserving as much subchondral bone as possible.


Assisted motion was initiated immediately, active-assisted motion started after 6 weeks and strengthening initiated at 12 weeks after surgery.
The Simple Shoulder Test (SST) score improved from a mean of 4.6±2.8 before surgery to 10.5±2.2 after surgery. This improvement averaged 80.6% of the maximum possible improvement. 85.1% of patients reached the minimal clinically important difference for the SST. Male sex and not having prior shoulder surgery were significantly associated with better clinical outcomes. Age, preoperative shoulder motion, and Walch glenoid classification were not associated with the outcomes.
5 patients underwent revision arthroplasty for pain; 3 had positive cultures for Cutibacterium at the time of revision. An additional 3 were dissatisfied at final follow-up without undergoing revision arthroplasty. Of these eight, seven had a history of prior shoulder surgery.
Medialization of the humeral head center of rotation averaged 0.56 mm/yr. No radiographic measure was associated with long-term clinical outcomes.
This year, these same authors published Comparison of Humeral-Head Replacement with Glenoid-Reaming Arthroplasty (Ream and Run) Versus Anatomic Total Shoulder Arthroplasty A Matched-Cohort Study in which they compared the outcomes of RnR to anatomic total shoulder arthroplasty (aTSA) using a retrospective matched-cohort study of 110 patients who underwent aTSA and 57 patients who underwent RnR, all procedures were performed by the same surgeon. The choice between the two procedures was made by joint patient-surgeon decision making after discussion of both alternatives. Of note, the same rehabilitation program was used for both procedures.
Propensity matching was performed using 21 preoperative variables.
Thirty-nine patient pairs were matched. All patients were male, with a mean age of 58.6 ± 7.3 years and a mean follow-up 4.4 ± 2.3 years.
Patients having aTSA improved their SST scores from 4.1 to 10.9. The percent of maximum possible improvement in the SST was 85.3%.
Patients having RnR improved their SST scores from 4.7 to 10.3.The percent of maximum possible improvement in the SST was 80.5%.
In a mixed-effects model analysis, arthroplasty type was not associated with outcome. There were no significant differences in the percentages of patients who achieved the minimal clinically important difference, substantial clinical benefit, or patient acceptable symptom state thresholds for the SST, ASES, and VAS for pain at ≥5 years. There were no differences between the two groups for health related quality of life measures.
After aTSA two patients underwent revision arthroplasty for glenoid loosening, at 9.2 and 14 years, and both were converted to hemiarthroplasty. At revision, cultures were positive for C. acnes for 1 patient, and negative for the other.
Comment: These two studies demonstrate that both RnR and aTSA are valuable procedures for patients with glenohumeral arthritis. In that revisions for glenoid component loosening typically occur years after aTSA, comparative studies with 10 or more years of followup will be necessary to better understand the relative advantages of the two approaches. The ream and run has now been around long enough that 10+ year followups are becoming available that show durability and applicability to complex glenoid pathologies without the need for 3D planning or augmented glenoid components.

In the meanwhile, the surgeons interested in the ream and run procedure are working to continually improve the outcomes of this plastic-free glenohumeral arthroplasty by optimizing patient selection, surgical technique, and identification of and prophylaxis for patients at risk for infection.
Follow on twitter: https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link).
Shoulder rehabilitation exercises (see this link).