
Thanks to Mihir Sheth, one of our current shoulder fellows, for helping with this post.
There is much current interest in the management of glenoid retroversion

The dysplastic glenoid is a malformation characterized by substantial (>25 degrees) retroversion of the glenoid articular surface. The posterior glenoid labrum is typically hypertrophic (red arrow).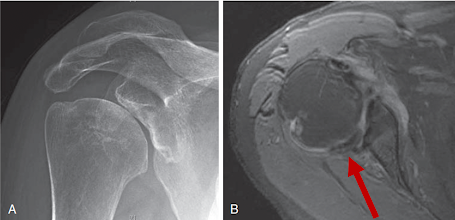

Publications on glenoid hypoplasia provide important lessons about glenoid retroversion.
There were no significant differences preoperatively among patients with type C and and type A1 glenoids with respect to sex, age, BMI, dominant side shoulder surgery, comorbidities, and length of followup.
A single surgeon performed all the arthroplasties using a cemented standard (nonaugmented) all-polyethylene glenoid (pegged or keeled) with a press-fit humeral stem. No effort was made to correct glenoid version through reaming or posterior bone graft. No patients underwent posterior capsulorrhaphy.
In the 29 patients with type C glenoids, there were 4 postoperative complications: aseptic glenoid loosening (2), isolated subscapularis failure (1), and superior migration of the humeral head (1). 1 patient required revision to reverse shoulder arthroplasty (RSA) and 1 patient for whom revision to RSA was recommended, giving an overall complication rate of 14% and revision rate of 7%.



This study found that Walch type C dysplastic glenoids - defined by severe retroversion without posterior humeral head decenting- were effectively and safely managed by standard anatomic total shoulder arthroplasty components without attempting to "correct" glenoid retroversion by high side reaming, bone graft, augmented glenoid components, or reverse total shoulder arthroplasty. The results of TSA for patients with retroverted displastic glenoids were not inferior to those with the anatomically simpler type A1 glenoids that did not have pathologic retroversion.
In the 29 patients with type C glenoids, there were 4 postoperative complications: aseptic glenoid loosening (2), isolated subscapularis failure (1), and superior migration of the humeral head (1). 1 patient required revision to reverse shoulder arthroplasty (RSA) and 1 patient for whom revision to RSA was recommended, giving an overall complication rate of 14% and revision rate of 7%.
In the 29 matched cohort patients with type A1 glenoids, there were 10 postoperative complications resulting in a 17% complication rate and a 12% revision rate. All 7 revisions were to RSA for aseptic glenoid loosening at a mean of 7 years from index TSA .
Clinical outcomes and radiographic outcomes were not different between the two groups.



This study found that Walch type C dysplastic glenoids - defined by severe retroversion without posterior humeral head decenting- were effectively and safely managed by standard anatomic total shoulder arthroplasty components without attempting to "correct" glenoid retroversion by high side reaming, bone graft, augmented glenoid components, or reverse total shoulder arthroplasty. The results of TSA for patients with retroverted displastic glenoids were not inferior to those with the anatomically simpler type A1 glenoids that did not have pathologic retroversion.
Hypoplasia of the glenoid. A review of sixteen patients Patients with glenoid dysplasia having high degrees of retroversion can be asymptomatic. Those with symptoms can benefit from a non-operative, patient-conducted rehabilitation program. A five years followup, most patients were able to return to work with resolution of symptoms. Progressive degenerative joint disease develops in some patients with the onset of refractory symptoms.
Shoulder arthroplasty for osteoarthritis secondary to glenoid dysplasia: an update Fourteen shoulders with advanced degenerative changes of the glenoid articular surface underwent total shoulder arthroplasty. Prior to insertion of the glenoid component, eccentric reaming of the anterior aspect of the glenoid was used to in attempt to change the glenoid version. Five of the fourteen total shoulders were revised: three for glenoid component failure and two for infection. The authors concluded that in cases of glenoid dysplasia, surgery should be avoided "unless the symptoms are extreme".


Nonsurgical treatment is reasonably successful in younger patients, but premature degenerative changes frequently occur. Although favorable results can be obtained with the use of anatomic arthroplasty, continued subluxation and glenoid component failure can lead to unacceptable outcomes.
The humeral is typically centered on a uniconcave glenoid articular surface (red line drawn perpendicular to the center of the glenoid arcticular surface). Because of the retroversion, most of the humeral head lies posterior to the plane of the glenoid (purple line).




A standard glenoid component can be inserted on the glenoid surface without changing glenoid version.

While this may result in perforation of the cortical bone of the anterior glenoid neck, this does not compromise glenoid component fixation, especially if a component with a fluted central peg is used.


Anatomic shoulder arthroplasty in Walch type C glenoid deformity: mid- to long-term outcomes reviewed 26 of 30 patients having hypoplastic glenoid morphology and glenohumeral osteoarthritis having an anatomic total shoulder arthroplasty (aTSA) followed up at an average of 8.5 years after surgery. The humeral head was typically centered on a retroverted glenoid as shown below.

Seven different surgeons performed the aTSAs. There was a substantial variability in the surgical technique: an augmented component was used in 9 patients; a standard component was used in 17. Of the 17 patients with non-augmented components, 9 underwent partial correction with asymmetrical reaming, 3 received a mini-inset glenoid component inserted without changing glenoid version, and 2 had an anteriorly offset humeral component.
Patients were clinically improved and generally satisfied with the outcome. No statistically significant differences in any outcome measure were observed between patients with augmented glenoid components and those with non-augmented glenoid components. One revision to reverse shoulder arthroplasty was performed for instability at 7 years postoperatively after a traumatic dislocation.
The changes in glenoid version from the use of partial correction or the use of augmented glenoid components was not stated, so the importance of modifying glenoid version is not known for these patients.
Comment: Taken together, these articles indicate that non-operative management is helpful in patients with glenoid dysplasia not having disabling arthritis. For those patients with disabling arthritis, total shoulder arthroplasty can be successful. At present, there is not good evidence supporting the need to "correct" glenoid retroversion in the shoulder with glenoid dysplasia (see Glenoid Version: Acceptors and Correctors).
It is worthwhile considering whether the approach used by some of these authors to the retroverted dysplastic glenoid with a centered humeral head - no version correction, standard anatomic glenoid component - might also be applicable to the type B3 glenoid which is also retroverted with a centered humeral head.
It is also worthwhile considering whether the application of 3 dimensional CT based planning to shoulders with glenoid dysplasia may lead surgeons to use more complex implants than those standard components successfully used in some of these studies.
You can support cutting edge shoulder research that is leading to better care for patients with shoulder problems, click on this link.
Follow on twitter: https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link).
Shoulder rehabilitation exercises (see this link).
Follow on twitter: https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link).
Shoulder rehabilitation exercises (see this link).