
In contrast to short and long stemmed humeral components, in which the humeral head is guided and supported by the humeral medullary canal,

short stemmed humeral components are positioned independently of the canal and supported by the bone of the humeral metaphysis. Each of the many different stemless designs has different metaphysial loading characteristics.

A comparison of revision rates for stemmed and stemless primary anatomic shoulder arthroplasty with all-polyethylene glenoid components: analysis from the Australian Orthopaedic Association National Joint Replacement Registry found that revision rates for stemmed and stemless humeral components did not significantly differ.






In a recent report of anatomic total shoulder arthroplasties, Radiographic comparison of eccentric stemmed vs. concentric stemless prosthetic humeral head positioning after anatomic total shoulder arthroplasty, stemless and stemmed anatomic total shoulder humeral implants had similar rates of reproducing satisfactory postoperative humeral head centers of rotation (COR); COR deviation occurred most commonly in the superomedial direction for both types of implants. Excessive humeral head height contributed to overstuffing for both stemmed and stemless implants.
Stemless components lead to improved radiographic restoration of humeral head anatomy compared with short-stemmed components in total shoulder arthroplasty studied 89 short stems and 140 stemless components. The mean COR shift for short stems was 2.7 mm compared with 2.1 mm for stemless implants. The percentage of short-stem implant patients with a >2 mm COR difference from native was 66.0% compared with 47.4% for stemless. The percentage of short-stem patients with a >4 mm COR difference from native was 17.0% compared with 3.0% for stemless.
See also Stemless total shoulder - are the clinical outcomes better than those with stemmed implants?
Selection and positioning of the humeral component - usually free hand without 3D CT planning or guidance.
With the stemless humeral component, the dimensions of the humeral component (diameter of curvature and thickness) are selected by the surgeon to create the desired anatomy and stability provided by the humeral articular surface. The position of the selected humeral component is determined by the bone cut at the proximal humerus. Most often this cut is made "free hand" at the anatomical neck after the osteophytes have been resected, extending from the cuff insertion superiorly to the capsular reflection inferiorly - roughly 135 degrees with the long axis of the shaft and at 30 degrees of retroversion (see this video and this video).

As shown in the case below, an oversized implant can be cause of joint overstuffing, leading to shoulder stiffness and pain.

As shown in the cases below, overstuffing can also result from an insufficient cut leading to improper positioning.


On the other hand, an over aggressive humeral cut can lead to weakness and instability from understuffing.

The authors of Concordance of Preoperative 3D Templating in Stemless Anatomic Total Shoulder Arthroplasty found that preoperative planning using Blueprint 3D Planning Software (Wright Medical Group) was of limited value in predicting the the size of the humeral head and nucleus implants actually used by the surgeon (38% and 60% concordance, respectively). Planned humeral head implants were more often oversized relative to their actual implanted size.
In a recent report of anatomic total shoulder arthroplasties, Radiographic comparison of eccentric stemmed vs. concentric stemless prosthetic humeral head positioning after anatomic total shoulder arthroplasty, stemless and stemmed anatomic total shoulder humeral implants had similar rates of reproducing satisfactory postoperative humeral head centers of rotation (COR); COR deviation occurred most commonly in the superomedial direction for both types of implants. Excessive humeral head height contributed to overstuffing for both stemmed and stemless implants.
Restoration of the native humeral anatomy during stemless anatomic total shoulder arthroplasty: a radiographic comparison of intramedullary versus freehand resection found that restoration of normal anatomy better for one surgeon who used an intramedullary guide than for a different surgeon who used a freehand cut. Whether this difference is due to the surgeon or the technique is unclear.

The authors of Stress shielding following stemless anatomic total shoulder arthroplasty found that with the Sidus Zimmer Biomet stemless component, 41% of shoulders demonstrated stress shielding at 2 years postoperatively. 7% demonstrated severe stress shielding with 6 occurring along the medial calcar.

The authors of Short-term radiographic analysis of a stemless humeral component for anatomic total shoulder arthroplasty reported the two year radiographic outcomes for 54 patients receiving the Equinoxe Stemless; Exactech. Stress shielding was observed in 4 patients (7%) with the medial calcar being the most common location of stress shielding. Three of the 4 patients had evidence of partial resorption while 1 patient (25%) had evidence of complete resorption.
Proximal humeral bone loss in stemless shoulder arthroplasty: potential factors influencing bone loss and a new classification system. found that women patients were more likely to experience bone loss after stemless arthroplasty.
Fixation and Loosening - some new variables to content with
Most articles show minimal early and mid-term rates of stemless humeral component loosening. A few recent studies are of interest in this regard.
Early fixation of the humeral component in stemless total shoulder arthroplasty : a radiostereometric and clinical study with 24-month follow-up obtained radiostereometric analysis radiographs in 24 patients at one day, six weeks, six months, one year, and two years after stemless arthroplasty. Median translation of the implant along the x, y, and z axes was less than 0.2mm. Rotation around the x, y and z axes was less than 0.2 degrees. Overall, 20 prostheses stabilized within 12 months postoperatively. Four prostheses showed continuous migration between 12 and 24 months.
An in vitro model study, The effect of shoulder prosthesis stem length on failure due to torsional loading. A biomechanical study in composite humeri found that long-stem implants were significantly stiffer than short or stemless implants. Stemless implants had a lower yield torque. The failure mechanism of stemless implants was through metaphyseal cancellous bone, emphasizing the effect bone quality has on implant fixation.
Stemless reverse humeral component neck-shaft angle has an influence on initial fixation used a finite element model to examine the effect of the angle of the neck cut on bone-implant interface distraction after loading. With every 5° decrease in neck-shaft angle, there was an average 17% increase in bone-implant distraction. Lower, more varus, neck-shaft angles increased bone-implant distractions with simulated activities of daily living.

Short term results of anatomic stemless shoulder replacement with peripheral neck fixation used a design combining central and peripheral fixation of the stemless implant to achieve stronger fixation at the humeral anatomic neck level.

A Comparison of Operative Time and Intraoperative Blood Volume Loss Between Stemless and Short-stem Anatomic Total Shoulder Arthroplasty: A Single Institution's Experience
The median surgical time for the stemless cohort was 111 minutes versus 137 minutes for the stemmed cohort.
Surgical time and outcomes of stemmed versus stemless total shoulder arthroplasty
The average operative time was 24 minutes less in the stemless cohort compared with the stemmed cohort (104 minutes vs. 128 minutes
Stress shielding - a different loading environment for the humerus
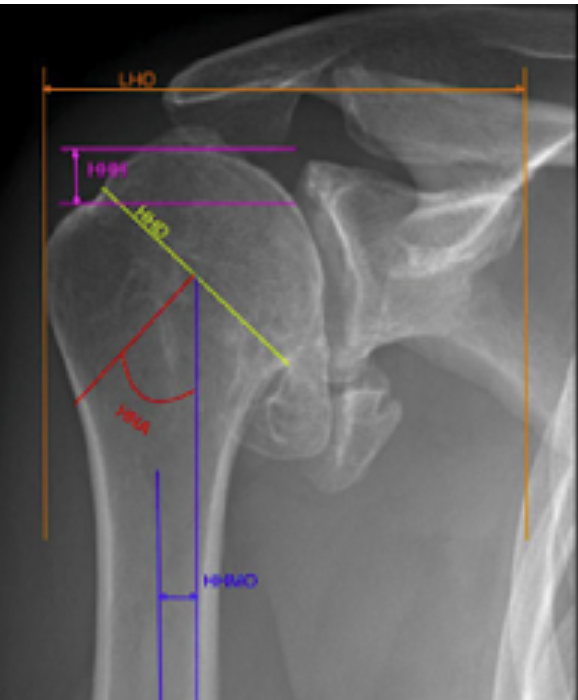
With stemmed implants, loads applied to the humeral head are distributed by the stem to the humeral diaphysis. Techniques such as impaction grafting can help spread out this distribution, resulting in reduced stress shielding (https://pubmed.ncbi.nlm.nih.gov/31272887/). However, with stemless humeral arthroplasty, loads applied to the humeral head are distributed to the humeral metaphysis (blue rectangle), bypassing the humeral cortex unless there is contact between the head and humeral neck cut (red arrows); the degree of cortical loading is a function of implant design and surgical technique.


The authors of Short-term radiographic analysis of a stemless humeral component for anatomic total shoulder arthroplasty reported the two year radiographic outcomes for 54 patients receiving the Equinoxe Stemless; Exactech. Stress shielding was observed in 4 patients (7%) with the medial calcar being the most common location of stress shielding. Three of the 4 patients had evidence of partial resorption while 1 patient (25%) had evidence of complete resorption.
While the authors of these articles noted no short term effects of the observed stress shielding, the degree of progression with time and the long term consequences are undetermined.
Most articles show minimal early and mid-term rates of stemless humeral component loosening. A few recent studies are of interest in this regard.
Early fixation of the humeral component in stemless total shoulder arthroplasty : a radiostereometric and clinical study with 24-month follow-up obtained radiostereometric analysis radiographs in 24 patients at one day, six weeks, six months, one year, and two years after stemless arthroplasty. Median translation of the implant along the x, y, and z axes was less than 0.2mm. Rotation around the x, y and z axes was less than 0.2 degrees. Overall, 20 prostheses stabilized within 12 months postoperatively. Four prostheses showed continuous migration between 12 and 24 months.
An in vitro model study, The effect of shoulder prosthesis stem length on failure due to torsional loading. A biomechanical study in composite humeri found that long-stem implants were significantly stiffer than short or stemless implants. Stemless implants had a lower yield torque. The failure mechanism of stemless implants was through metaphyseal cancellous bone, emphasizing the effect bone quality has on implant fixation.


Infection risk - might it be lower with stemless?
The risk of infection complicating shoulder arthroplasty may be related to the time the wound is open. Stemless arthroplasty appears to be associated with shorter surgical times as shown in the studies below.
The median surgical time for the stemless cohort was 111 minutes versus 137 minutes for the stemmed cohort.
Surgical time and outcomes of stemmed versus stemless total shoulder arthroplasty
The average operative time was 24 minutes less in the stemless cohort compared with the stemmed cohort (104 minutes vs. 128 minutes
Other factors might lower infection risk for stemless implants (N.B. these are pure speculation):
(1) Stemless components contain less titanium alloy, which is a favorite surface for biofilms
What does an infected biofilm on a titanium implant look like?
Biofilms on titanium - the race to the surface
(2) Stemless components do not require instrumentation of the medullary canal, which can introduce bacteria to it. Perhaps the hypovascularized adult medullary canal is less aerobic than the well-vascularized metaphysis. Cutibacterium can thrive in an aerobic environment.
Comment: Stemless components require surgeons to substantially change their thinking about and approach to shoulder arthroplasty. Their use introduces new variables that are different than those encountered with short or standard length stems. Time and well-done clinical studies will clarify how stemless components can be used most effectively and safely.
You can support cutting edge shoulder research and education that are leading to better care for patients with shoulder problems, click on this link.
Follow on twitter: https://twitter.com/RickMatsen or https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link).
Shoulder rehabilitation exercises (see this link).