
Thus the question, "Short stemmed humeral components - do they solve old problems or create new ones?"
The intramedullary anatomy of the proximal humerus is irregular and highly variable among patients.


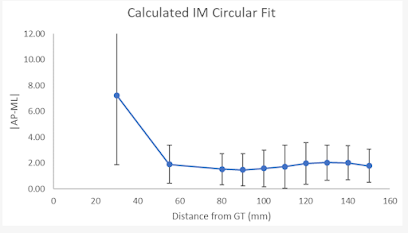
A Radiographic Analysis of Proximal Humeral Anatomy in Patients with Primary Glenohumeral Arthritis and Implications for Press-Fit Stem Length pointed out that short stems in total shoulder arthroplasty are associated with higher rates of malalignment and loosening compared to standard length stems. A study of CT scans on 99 consecutive patients undergoing shoulder arthroplasty documented this variability. The chart below plots the difference between the anteroposterior and mediolateral dimensions of the canal as a function of the distance down the humerus from the greater tuberosity.
 As shown in Short stem humeral components in reverse shoulder arthroplasty: stem alignment influences the neck-shaft angle this inconstant anatomy can result in variable positioning of a short stemmed component in the canal.
As shown in Short stem humeral components in reverse shoulder arthroplasty: stem alignment influences the neck-shaft angle this inconstant anatomy can result in variable positioning of a short stemmed component in the canal. 


This can result in variable positioning of the proximal aspect of the component as well as point loading of the diaphysial canal (red arrows).

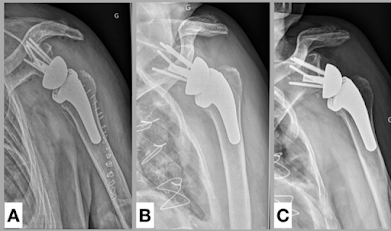
Lack of a good fit in the variable humeral canal can result in high rates of loosening of short stemmed humeral components as demonstrated in Radiographic evaluation of short-stem press-fit total shoulder arthroplasty: short-term follow-up. Symptomatic aseptic loosening of a short humeral stem following anatomic total shoulder arthroplasty assessed 184 shoulders that received TSA with a grit-blasted, rectangular short humeral stem without ingrowth coating. The rate of symptomatic aseptic humeral loosening in this series was 10.9%, with 5.4% undergoing revision surgery. Note the components below have subsided into varus with lateral diaphysial erosion.


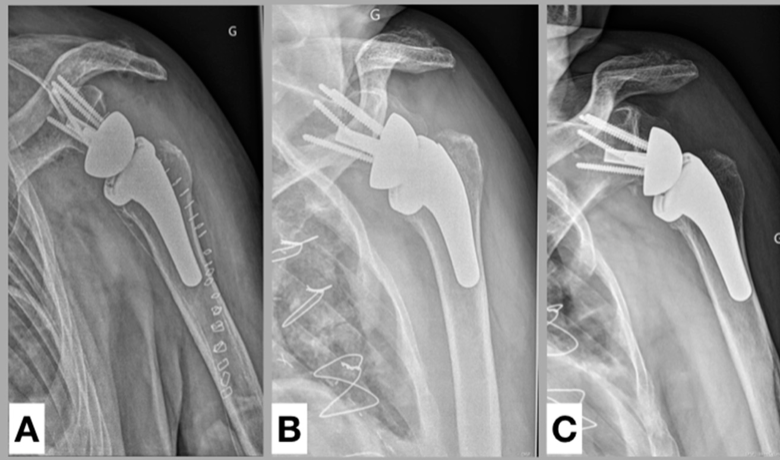
Subsidence of Uncemented Short Stems in Reverse Shoulder Arthroplasty-A Multicenter Study reviewed 139 patients at a minimum follow-up of 12 months. The average subsidence was 1.4 mm. Subsidence of >5 mm was present in 15 patients (11%). Note once more that the component has subsided into varus with lateral diaphysial erosion.
It appears that without the stabilizing effect of a standard length stem, loading of a short stemmed component can cause it to collapse into varus.

Attempts to obtain secure press-fit fixation of a short stemmed component in the humeral canal can increase the risk of periposthetic fractures as seen in Surgical fixation of periprosthetic humeral shaft fracture about a short-stem anatomic total shoulder arthroplasty with a proximal humeral locking plate: surgical technique and report of 3 cases



The intramedullary anatomy of the proximal humerus is irregular and highly variable among patients.

As a result, no short stem humeral implant design can be expected to conform to it.



Similar findings are reported in Short Humeral Stems in Shoulder Arthroplasty



Lack of a good fit in the variable humeral canal can result in high rates of loosening of short stemmed humeral components as demonstrated in Radiographic evaluation of short-stem press-fit total shoulder arthroplasty: short-term follow-up. Symptomatic aseptic loosening of a short humeral stem following anatomic total shoulder arthroplasty assessed 184 shoulders that received TSA with a grit-blasted, rectangular short humeral stem without ingrowth coating. The rate of symptomatic aseptic humeral loosening in this series was 10.9%, with 5.4% undergoing revision surgery. Note the components below have subsided into varus with lateral diaphysial erosion.


It appears that without the stabilizing effect of a standard length stem, loading of a short stemmed component can cause it to collapse into varus.



Lack of evenly distributed loading of the humerus by the stem can result in stress shielding.

Mid-term radiological results of a cementless short humeral component in anatomical and reverse shoulder arthroplasty found that in 100 shoulder arthroplasties evaluated at a mean of 3.8 years, greater tuberosity stress shielding was noted in 14 shoulders and medial calcar resorption was noted in 23 shoulders.
Mid-term results of anatomical total shoulder arthroplasty for primary osteoarthritis using a short-stemmed cementless humeral component found that 40% of the shoulders developed substantial bone loss in the proximal humerus between four and seven years of follow-up.

3 female patients with GB stems had gross loosening of their humeral components before 1 year. Radiolucent lines around the humeral component were found in 5.9%. Osseous resorption at the medial cortex was noted in 9.3%. Of patients with PPC stems, no patients were observed to have radiolucent lines compared with 8.2% in the GB group,
If the quality of bone of the proximal humerus is sufficient for fixation, a thinner short stem has a reduced risk of stress shielding because of the smaller filling ratio (see The effect of short-stem humeral component sizing on humeral bone stress and The effects of length and width of the stem on proximal humerus stress shielding in uncemented primary reverse total shoulder arthroplasty and Implications of humeral short-stem diametral sizing on implant stability)


It has been suggested that these short stemmed humeral components have the advantages of more bone stock preservation, less stress shielding, less diaphyseral stress risers, lower risk of fracture, easier component extraction during revision, and better humeral head positioning that is independent of the orthopaedic humeral axis. (see Short Humeral Stems in Shoulder Arthroplasty).



Follow on twitter: https://twitter.com/RickMatsen or https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link).
Shoulder rehabilitation exercises (see this link).
Proximal humeral bony adaptations with a short uncemented stem for shoulder arthroplasty: a quantitative analysis reported a retrospective study of 183 shoulder arthroplasties evaluated at 2-year follow-up. Medial cortical narrowing was found in 72.6% of cases and was severe (>50%) in 4.4%. Medial metaphysis thinning was found in 46.4% of cases and was severe in 3.3%. Lateral metaphysis thinning was found in 9.8% of cases and was severe in 2.8%. 



Clinical and radiographic outcomes after total shoulder arthroplasty with an anatomic press-fit short stem identified 118 TSAs completed with press-fit short stem and minimum 2-year follow-up; 85 of these patients had a grit-blasted (GB) short stem placed, whereas 33 patients had short stems with proximal porous coating (PPC).


The design of the short stem can have a dramatic effect on stress shielding. Radiographic changes differ between two different short press-fit humeral stem designs in total shoulder arthroplasty found that the rate of medial calcar osteolysis varied from 71% to 28.5% between two different stem designs.



3 female patients with GB stems had gross loosening of their humeral components before 1 year. Radiolucent lines around the humeral component were found in 5.9%. Osseous resorption at the medial cortex was noted in 9.3%. Of patients with PPC stems, no patients were observed to have radiolucent lines compared with 8.2% in the GB group,


However, as pointed out above in Short stem humeral components in reverse shoulder arthroplasty: stem alignment influences the neck-shaft angle, smaller short stems are more likely to be malaligned.
All of the above relates to the challenges in alignment in the AP plane. However, there are problems with controlling the position of the stem in the axillary plane as well. In the case below, one can see that posterior displacement of the stem in the humeral canal as well as posterior angulation of the implant have combined to yield posterior decentering of the head in the glenoid.

Comment: A wide variety of short stem humeral components are on the market, some of which are shown below. As can be seen, they come in a wide variety of stem shapes, stem sizes and stem surfaces.
The question is "which short stem design is being compared to what standard stem?" In the figure below one can consider the amount of bone removed, the potential for stress shielding, the presence of stress risers, the potential fracture risk, the potential ease of prosthesis exchange, and the humeral head component positioning for two short stemmed designs (left and right) in comparison to a smooth standard length stem inserted with impaction autografting (center).



The goal of this post is to call attention to the special considerations that relate to the use of a short stemmed humeral component, recognizing that its fit, stability and loading of the humeral canal are all different than those for a standard length stem.
You can support cutting edge shoulder research and education that are leading to better care for patients with shoulder problems, click on this link.
Follow on twitter: https://twitter.com/RickMatsen or https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link).
Shoulder rehabilitation exercises (see this link).