In contrast to the situation in an anatomic shoulder arthroplasty (below left), the center of rotation (center of yellow circle) in a reverse total shoulder (below right) is not closely aligned with the humeral medullary canal (red line). This results in a rotational moment arm (blue line) and a bending force each of which can contribute to loosening of the humeral stem in the humeral canal.

These loosening factors need be resisted by secure and durable fixation of the prosthesis to bone.
Recently there has been interest in short stemmed reverse humeral components.
However the short stem places the implant at risk for shift in component position as shown below.

Some have tried to manage this tendency for loosening by using tight fitting components, but these can increase the risk of stress shielding as shown below.



The authors used cadaveric specimens to evaluate the effect of three-dimensional volumetric humeral canal fill ratios of reverse shoulder arthroplasty short and standard stems on the biomechanical stability and bone deformations in the proximal humerus.
They compared standard stems inserted with low and high filling ratios and short stems inserted with low and high filling ratios.

The specimens were cyclically loaded while optical recording allowed for spatial implant tracking and the quantification of cortical bone deformations in the proximal humerus.
Both short and standard-length stem RSA humeral components implanted with a low canal filling ratio maintain dynamic bone loading in the medial calcar of the humerus similar to the native bone tested. This dynamic bone loading is desirable in the prevention of bone losss from stress shielding. Thus high canal fill ratios ( > 0.72) may correlate with the severity of bone resorption in the clinical setting.
However, short stems implanted with a low filling ratio (< 0.72) have an increased risk for implant tilt and subsidence compared to those inserted with high filling ratios or standard length stems. Short stems inserted with higher filling ratios and standard length stems implanted with low or high filling ratios demonstrated higher primary stability.

A conclusion from the foregoing is that short stems are at risk for stress shielding if they are inserted with high filling ratios, and at risk for loosening (tilt and subsidence) if they are inserted with low filling ratios.
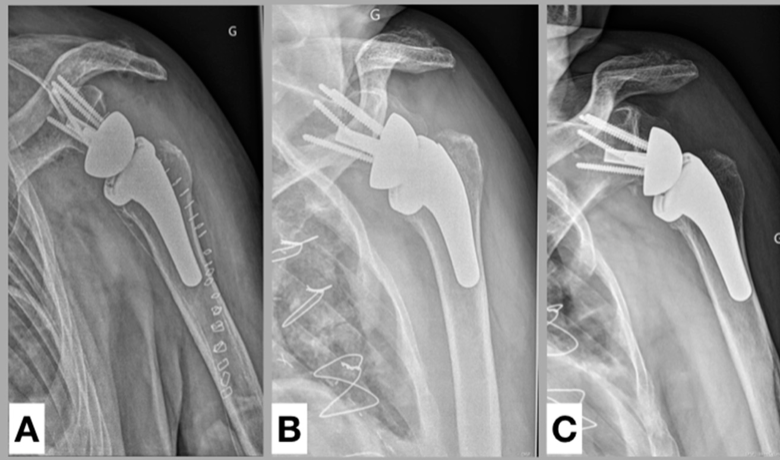
So, one can reduce the risks of stress shielding and component loosening through the use of a standard length smooth stem inserted with a low filling ratio as seen in the x-ray below with a stable humeral component and no bone resorption two years after reverse total shoulder arthroplasty. Secure fixation is achieved through impaction autografting.

You can support cutting edge shoulder research that is leading to better care for patients with shoulder problems, click on this link
Follow on twitter/X: https://x.com/RickMatsenFollow on facebook: https://www.facebook.com/shoulder.arthritisFollow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link)
Shoulder rehabilitation exercises (see this link).
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link)
Shoulder rehabilitation exercises (see this link).