




Here's an example of poor glenoid preparation.


that can result when a guide wire fixes the orientation of a cannulated reamer in an attempt to modify glenoid version (see How much does "corrective glenoid reaming" actually change version and is the version change of benefit ?)
Poor glenoid preparation cannot be remedied by placing cement between the bone and component - this cement will fracture, displace and leave the component unsupported, often in the critical posterior aspect of the joint.

In contrast to the guide wire and cannulated reamer ("A" below), the wireless approach uses a non-cannulated nubbed reamer ("B" below) that can be angulated so that the bony glenoid face is completely reamed to a single concavity with minimal bone removal.










Follow on twitter: https://twitter.com/RickMatsen or https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link).
Shoulder rehabilitation exercises (see this link).

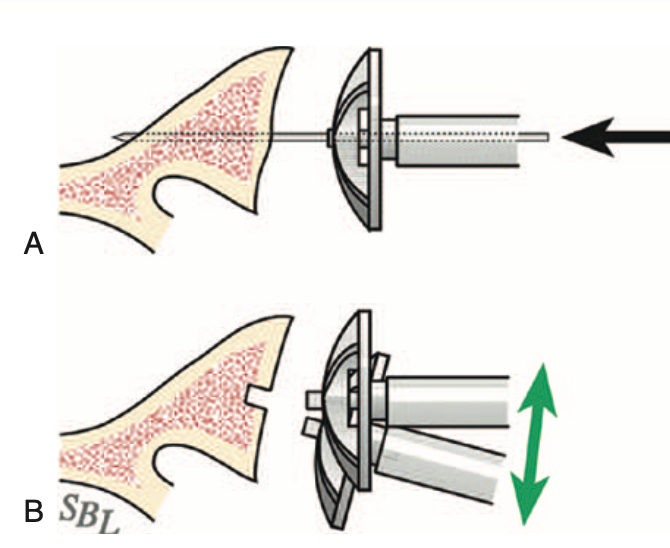
While reaming, the surgeon can adjust the angle of the reamer so that blades contact and ream the entire glenoid bone surface (green arrows below).


The adequacy of the reaming can be verified by using a round backed trial to see if it tips when loaded (upper figure) or if it is stable on the reamed glenoid surface (bottom figure).

Wireless reaming can be used with any implant system offering a nubbed reamer that can be inserted into a shallow hole in the center of the glenoid.


As described above, the surgeon can adjust the angle of the reamer so that blades contact and prepare the entire glenoid bone surface (green arrows below).

And again, the completeness and adequacy of the reaming can be verified by using a round backed trial to see if it tips when loaded or if it is stable on the reamed glenoid surface.

Below are the preoperative and postoperative axillary truth views from a patient who had wireless reaming for B2 glenohumeral pathology.

The wireless preparation of the glenoid does not require a preoperative CT scan.
It also reduces the risk of over reaming with loss of the glenoid bone stock needed to support the glenoid component as shown in the upper two figures below. (see Version Correction via Eccentric Reaming Compromises Remaining Bone Quality in B2 Glenoids: A Computational Study)

Thanks as always to Steve Lippitt for his wonderful art - often used, seldom acknowledged.
You can support cutting edge shoulder research and education that are leading to better care for patients with shoulder problems, click on this link.
Follow on twitter: https://twitter.com/RickMatsen or https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link).
Shoulder rehabilitation exercises (see this link).