There is a rapidly expanding number of humeral components being sold for anatomic arthroplasty.
Let's consider the features of a legacy "universal" anatomic humeral component system against which these newer alternatives can be compared.
The primary principles are (1) bone preservation, (2) avoidance of stress shielding, and (3) availability of humeral head options to manage the variations in arthritic pathoanatomy.
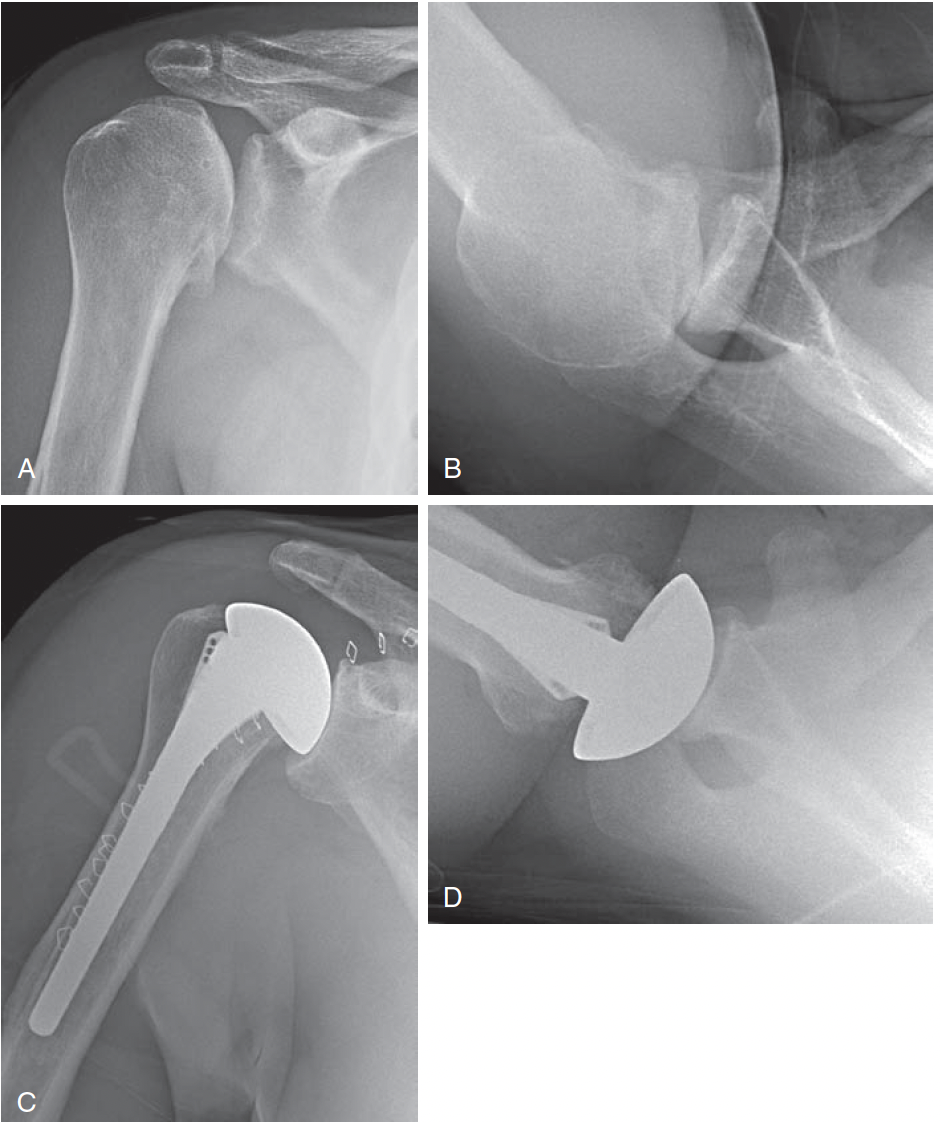
These goals can be achieved with a standard length smooth stem with a low filling ratio fixed with impaction grafting coupled with a versatile selection of heads, including eccentric and cuff tear arthropathy options. NB: the author has no ties with any implant company, so this is not a sales pitch, but rather a perspective gained from almost 50 years of practice in shoulder arthroplasty.
Bone preservation: the head cut is the same as for short stemmed and stemless
Bone is not removed from the canal by reaming
instead, a stem diameter is selected that is smaller than the internal diameter of the diaphysis, yielding a small filling ratio without violating the bone of the canal.
The irregular internal anatomy of the humerus
is fit to the stem using impaction grafting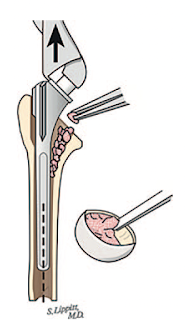
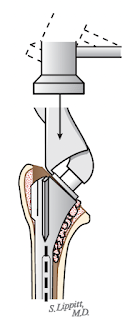
The security of this fixation obviates the need for ingrowth surfaces on the implant, which can complicate removal of the stem should it become necessary.
The bone graft spreads the load broadly across the interface between the stem and bone minimizing the risk of stress shielding.
Stress shielding can be a problem when an implant is fit tightly against the distal cortical bone.
The use of a thin stem enables proper seating of the component
.
avoiding the issue of incomplete seating that can be seen with a large stem
Because the shaft is not weakened, the thin stem with impaction grafting technique minimizes the risk of intraoperative and postoperative fractures.
The thin stem with impaction grafting can be applied to special situations, for example when a plate is retained to protect the humerus.
The thin stem with impaction grafting technique can be safely applied to osteopenic bone, without being concerned about the results of the "thumb test"
or the need for intraoperative conversion from a stemless to a stemmed component (see Pre-operative Metaphyseal Cancellous Bone Density is Associated with Intraoperative Conversion to Stemmed Total Shoulder Arthroplasty).
A single piece body
avoids the potential risk of corrosion, loosening and disassembly that can be an issue with mutlipart stems
Having the male taper on the head, rather than the body keeps it from blocking access to the glenoid
The prosthetic head should come in a wide variety of diameters of curvature to match different glenoid curvatures
Each head diameter of curvature should have different thicknesses
so that the soft tissue tension can be adjusted to meet the 40, 50, 60 rules
Eccentric / offset options should be available to manage excessive posterior translation
Extended articular surface options should be availabe to manage cuff tear arthropathy in CTA shoulders with retained active elevation.
These two non-anatomic strategies are difficult to accomplish with a stemless system.
Comment: There is a vast set of options available for the the humeral side of a glenohumeral arthroplasty. Surgeons seem to be switching from one to another to see which they like best.
The challenge is to determine which, if any, are of greater value (benefit/cost) to the patient than the legacy approach presented above. Long term studies will be required, such as that presented by the population-based Australian Orthopaedic Association's National Joint Replacement Registry showing long term data for some of the options for treating primary osteoarthritis of the glenohumeral joint. Note the option that got gold.

You can support cutting edge shoulder research that is leading to better care for patients with shoulder problems, click on this link.
Follow on twitter: https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link).
Shoulder rehabilitation exercises (see this link).