I hope you enjoy the Hidden Brain as much as I do.
A recent post Do less. points out that the human drive to invent new things has led to pathbreaking achievements in medicine, science and society. But our desire for innovation can keep us from seeing one of the most powerful paths to progress: subtraction. Sometimes the best way forward involves removing, streamlining and simplifying things.
One of the examples given is that while training wheels on a kid's bike seem like a good innovation, it enabled the child to ride without learning to balance.
It turns out that a better way to teach a kid to ride is to subtract the pedals and training wheels and - voila - the balance bike.

I'm also a big fan of the ASES podcast. A recent program, Balloon vs. Tuberoplasty, reviewed options for managing irreparable rotator cuff tears, including superior capsular reconstruction, subacromial balloons, partial repairs, tendon transfers, and "biologic" tuberoplasty. The panel concluded that while there were "non-inferiority" studies and case reports, no surgical procedure was the clear favorite. As an example, a recent case series, Arthroscopic Subacromial Balloon Spacer for Massive Rotator Cuff Tears Demonstrates Improved Shoulder Functionality and High Revision-Free Survival Rates at Minimum 5-Year Follow-up, combined debridement with the placement of a subacromial balloon in 61 patients. 10 were lost to follow-up over 3 years. Of the remaining 51, 9 were lost at the latest follow-up. 17% required revisions within two years. Constant-Murley total scores increased significantly (27 to 69). 10% were highly satisfied, 48% were satisfied, and 43% were dissatisfied.
The podcast concluded with Justin Griffin saying, "There may be a future where we figure out a way to retrain the deltoid in the setting of a massive cuff tear that does not require any procedures." - an example of innovation by subtraction.
Many shoulders with chronic irreparable cuff tears (including my own) are comfortable and functional. For patients with chronic irreparable cuff tears and problematic weakness, there is the opportunity to use a simple exercise to retrain the deltoid, which is the primary source of shoulder power no matter what other treatments are considered.
Patients with irreparable cuff tears can have painful subacromial crepitus, which can be identified by placing the examiner's finger just anterior to the acromion while the shoulder is moved in rotation and elevation. As mentioned in the ASES podcast, many surgical procedures have been advocated for such a patient, yet there are very few studies that compare these methods with each other.
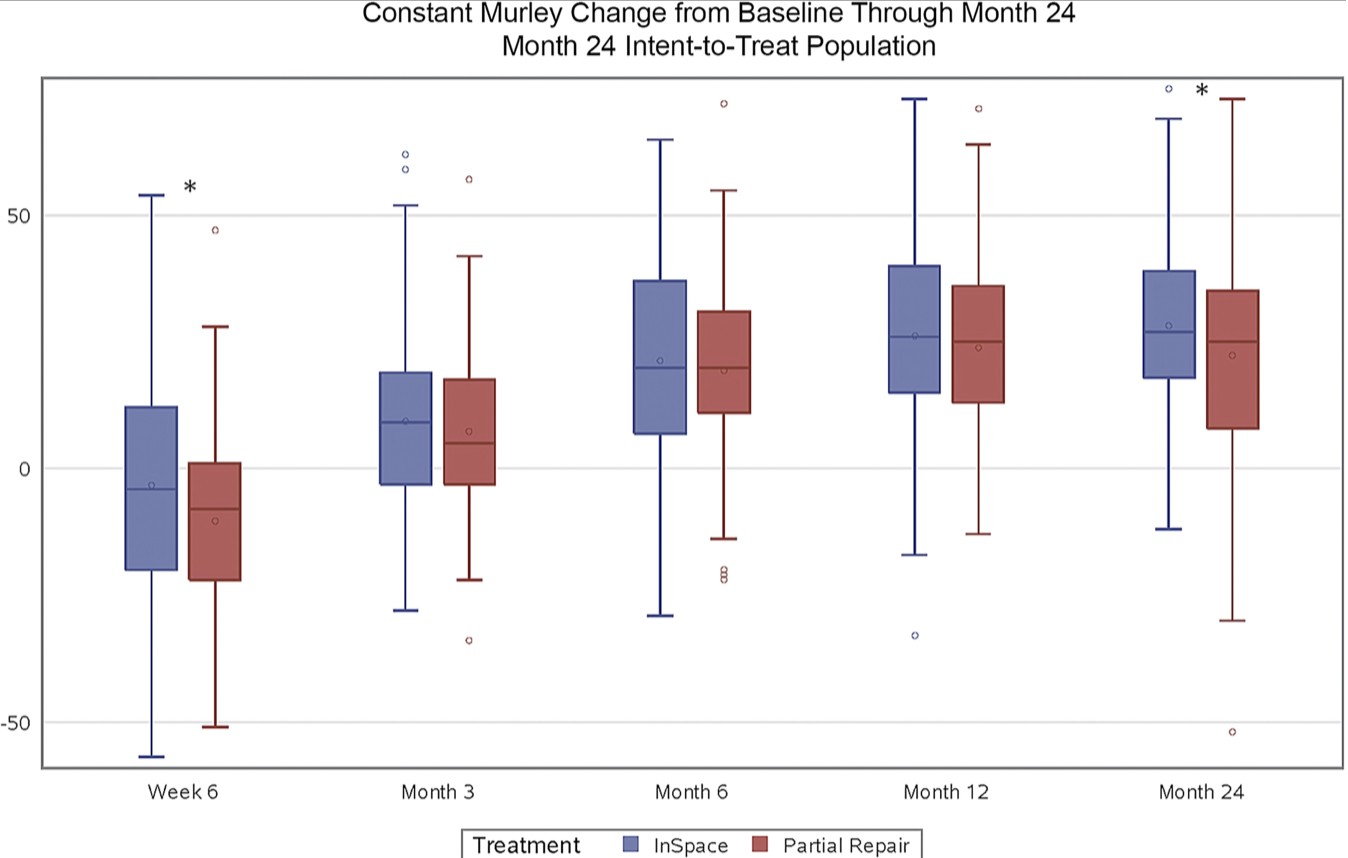
The authors of Comparison of Multiple Surgical Treatments for Massive Irreparable Rotator Cuff Tears in Patients Younger Than 70 Years of Age network meta-analysis to analyze comparative studies of surgical treatment options for massive irreparable cuff tears - without glenohumeral arthritis or pseudoparalysis - in patients <70 years of age. The treatments included debridement; arthroscopic bridging graft; arthroscopic partial repair; superior capsular reconstruction; long head of biceps augmented superior capsular reconstruction; InSpace balloon placement; tendon transfer; and reverse shoulder arthroplasty.
A total of 23 studies met the inclusion criteria, with 1178 patients included in the analysis. The mean weighted age was 62.8 years; 48.2% were men, mean follow-up was 28.9 months. There were no significant differences between groups in regard to sex or age.
The treatments were ranked using the the P-score - an estimate of the likelihood that the investigated treatment is the ideal method for an optimal result for each of the different outcome measures, where 0 is least effective and 1 is most effective.
Unfortunately most studies did not evaluate treatment with simple debridement in comparison to more complex procedures. However for studies that did, debridement had the highest P-score, as shown below.

Forrest plot for Constant Score:

Forrest plot for range of active forward flexion:
This network meta-analysis found that simple debridement was the most effective procedure in significantly improving Constant score and active flexion for individuals with massive irreparable cuff tears when it was compared to other more complex surgical modalities.
Comment: Debridement is a component of most procedures performed for irreparable cuff tears. Debridement alone subtracts away the other possible surgical elements (balloons, grafts, partial repair). It has the important advantages of not requiring any post-surgical down time and of not burning bridges for other procedures should it not yield the desired result. Furthermore it is the least costly in comparison to grafts, balloons, and partial repairs and avoids the possible complications of these procedures.
We refer to our approach to debridement as the "smooth and move procedure" emphasizing the goals of smoothing the articulation between the coracoacromial arch and the proximal humerus and initiating passive and active motion following the procedure. We have found this procedure to be effective not only as a primary procedure for patients with irreparable cuff tears, but also as a revision procedure for patients with failed prior attempts at surgical reconstruction.
Elements of this technique include (1) preserving the integrity of the deltoid and coracoacromial arch, (2) preserving the long head of the biceps unless it is frayed or dislocated, (3) removing hypertrophic bursal tissue, (4) trimming the rough edges of the reaming cuff, (5) resecting the prominent portions of the greater tuberosity, (6) manipulating the shoulder to eliminate any capsular tightness, and (7) starting motion exercises immediately after surgery.
The surgical technique and the outcomes of two patients having the smooth and move after failed cuff reconstruction attempts is shown in this link.
Two publications present the outcomes for this procedure:
Significant improvement in patient self-assessed comfort and function at six weeks after the smooth and move procedure for shoulders with irreparable rotator cuff tears and retained active elevation
Treatment of irreparable cuff tears with smoothing of the humeroscapular motion interface without acromioplasty
Comment to shoulderarthritis@uw.edu
You can support cutting edge shoulder research that is leading to better care for patients with shoulder problems, click on this link