
These authors used a cadaver model to help understand role the long head of the biceps tendon (LHBT) in glenohumeral stability.
They found that loading the biceps tendon at 30 and 60 degrees of forward flexion increased glenohumeral stability when posteriorly directed loads were applied.
Comment: The stabilizing effect of the biceps tendon is demonstrated by one of the common mechanisms for a SLAP injury in which posterior force applied to the joint avulses the origin of the long head from the glenoid.

We find it helpful to consider the analogy of a monorail in which the train is stabilized by sliding along a fixed track

The biceps "rail" is secured to the superior glenoid rim.
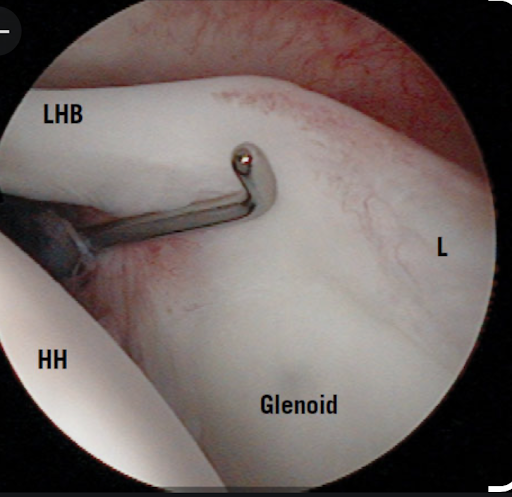
The humerus is secured on the rail by the biceps sheath and the transverse humeral ligament as shown in this arthroscopic view

and in this illustration from our late colleagues John Clark and Doug Harryman's classic "Tendons, ligaments, and capsule of the rotator cuff. Gross and microscopic anatomy"

The biceps sheath and the transverse humeral ligament keep the humerus riding along the rail of the biceps tendon - the stabilizing effect of which becomes greater as the shoulder is elevated, bringing the transverse humeral ligament closer to the supraglenoid tubercle.

The role of the biceps tendon in stabilizing the shoulder is not only important for understanding the SLAP tear, but also in glenohumeral arthroplasty. For this reason, we preserve the long head tendon of the biceps in performing the ream and run (see this link or anatomic total shoulder (see this link) unless it is severely frayed or dislocated. While some surgeons (self-declared "biceps killers") routinely sacrifice the tendon at arthroplasty, in our experience the incidence of problems with a preserved biceps post arthroplasty is very low.
Follow on twitter: https://twitter.com/shoulderarth
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
How you can support research in shoulder surgery Click on this link.
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link)
Shoulder arthritis - x-ray appearance (see this link)
The smooth and move for irreparable cuff tears (see this link)
The total shoulder arthroplasty (see this link).
The ream and run technique is shown in this link.
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).


















