
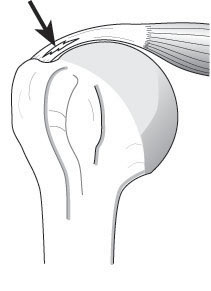
Detachment of the rotator cuff tendons from the greater tuberosity is often described as a rotator cuff tear. The word 'tear' suggests an acute process, such as tear in otherwise great blue jeans that can be easily repaired.

On the other hand, most cuff defects arise in tendons of suboptimal quality without an acute traumatic episode and may be better referred to as cuff wear, similar to defects in worn jeans that defy repair.

We emphasize the distinction in an article on rotator cuff failure in the New England Journal as well as in the text, The Shoulder, where we quote McLauhglin's admonition regarding 'rotten cloth to sew' in an Instructional Course Lecture: "The wise surgeon, realizing that he may find little but rotten cloth to sew, will operate only by necessity and make a carefully guarded prognosis. [There was complete agreement of the Panel on this point.]" See his 1962 article.
===
Check out the new Shoulder Arthritis Book - click here.
Use the "Search" box to the right to find other topics of interest to you.
You may be interested in some of our most visited web pages including:shoulder arthritis, total shoulder, ream and run, reverse total shoulder, CTA arthroplasty, and rotator cuff surgery as well as the 'ream and run essentials'
You may be interested in some of our most visited web pages including:shoulder arthritis, total shoulder, ream and run, reverse total shoulder, CTA arthroplasty, and rotator cuff surgery as well as the 'ream and run essentials'



































{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}