
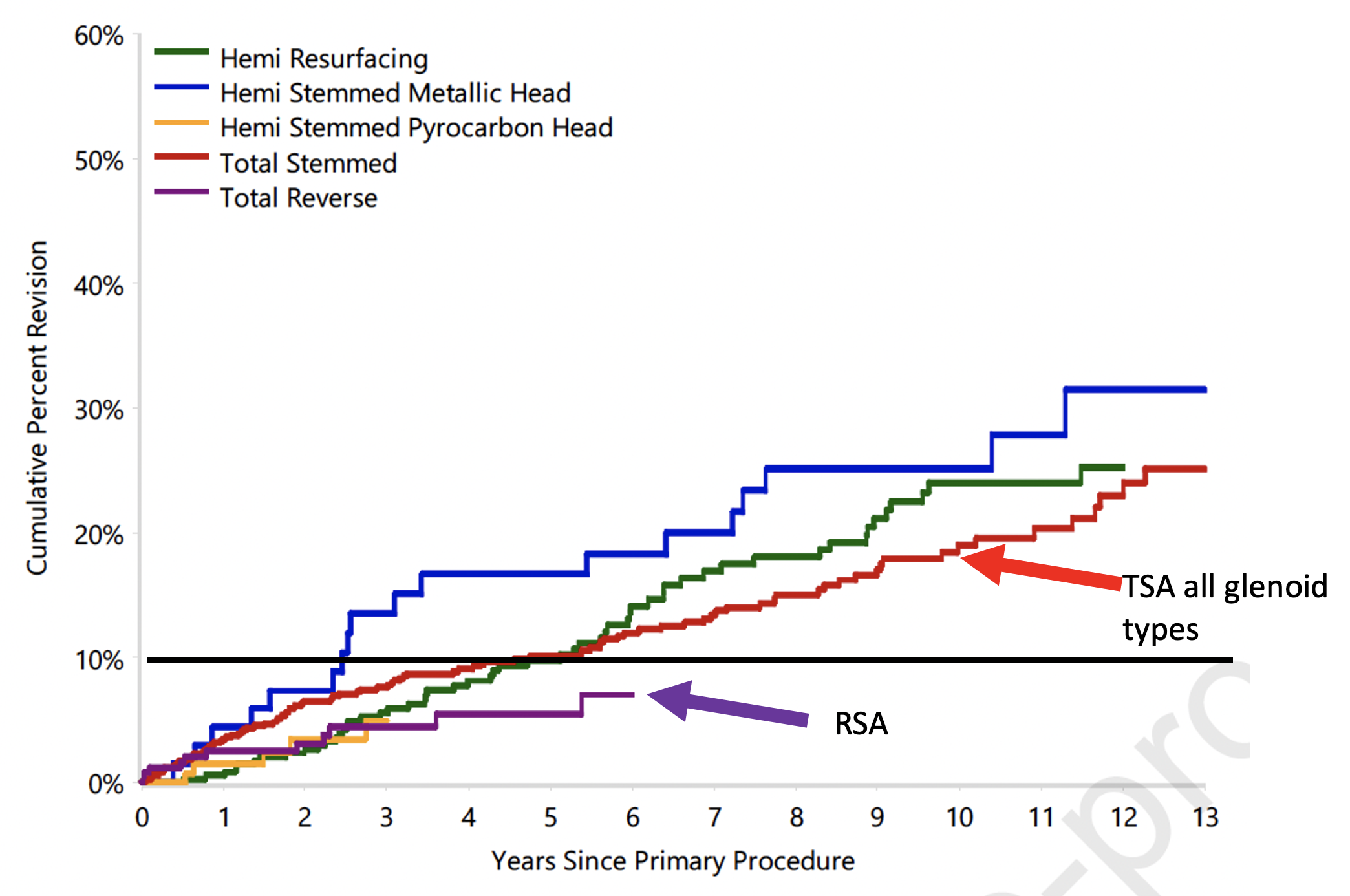
The authors of Survivorship of shoulder arthroplasty for young patients with osteoarthritis: An Analysis of the Australian Orthopaedic Association National Joint Replacement Registry sought to compare the survivorship and reasons for revision in 1,564 patients aged <55 years with a primary diagnosis of osteoarthritis having one of five types of shoulder arthroplasty between April 2004 to December 2020: total shoulder arthroplasty (TSA)(45.7%), hemiarthroplasty resurfacing (HRA) (23.1%), hemiarthroplasty stemmed metal head (HSMH)(4.5%), reverse total shoulder arthroplasty (RTSA)(16.6%) and hemiarthroplasty stemmed pyrocarbon head (HSPH) (10.2%) (see Does the innovation of pyrocarbon humeral head prostheses add value for young patients with arthritis?).
The cumulative percent revision for the different types of implant are shown below,
These results can be compared to those of another study based again on the Australian Orthopaedic Joint Replacement Registry for patients having shoulder arthroplasty during the same time period April 2004 to December 2020) Total Shoulder Replacement Stems in Osteoarthritis – short, long or reverse? An analysis of the impact of cross-linked polyethylene. The ages of these patients were not reported.

If attention is focused on RSA and stemmed TSA, one can see that the cumulative percent revision for RSA is similar in the two analyses. However, the cumulative percent revision for the stemmed TSA is about five times higher in the first study, even though both analyses were done on Australian Orthopaedic Joint Replacement Registry data from the same time period. There are several possible reasons for the observed differences.
(1) The first analysis apparently included glenoid components of all types. A commonly used system during the period of analysis in the Australian registry was the Lima SMR L1 and L2 which is known to have a high revision rate (see red box below).

The SMR L1 and L2 had revision rates 5 to 10 times that of an all-polyethyene glenoid. Inclusion of failures with this prosthesis would greatly exaggerate the cumulative revision rate for TSA in the first study.The SMR L1 and L2 were recalled in 2015 (see this link).

(2) The second analysis separated the revision rates for all-polyethylene glenoid components into cross-linked (XLPE) and non cross-linked (non XLPE). As can be seen in the second graph above, the cumulative revision rates for XLPE were about half of those for non XLPE.
(3) The patients in the two analyses were different: in the first patient age was <55 years and the patients were predominantly male. The patient ages and sex are not presented in the second analysis.
Comment: These two analyses provide important information on the revision rates for different types of arthroplasty in a defined national population. A comparison of the two studies indicates that the glenoid prosthesis type matters in the study of shoulder arthroplasty revision rates. Future analyses would be most meaningful if the important characteristics of the implants, patients and shoulders were identified so that subgroups could be studied separately.
Comparing these two studies reveals characteristics of the national arthroplasty practice in Australia, where there has been substantial use of metal backed glenoids as well as pyrocarbon humeral heads. These differences merit consideration when comparing the revision rates to other practice settings.
There are many options for managing arthritis in the challenging young patient with arthritis. While revision rates are an important metric, others important measures include the improvement in patient self-assessed comfort and function, patient satisfaction, the ability of patients to return to their desired activity levels, and the potential for revision surgery if the first arthroplasty fails.
Much clinical research remains to be done.
Follow on twitter: https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link).
Shoulder rehabilitation exercises (see this link).