
These authors reviewed some of the issues surrounding subscapularis tendon management at shoulder arthoplasty. Options include tendon tenotomy, peel, lesser tuberosity osteotomy, and even subscapularis sparing techniques. Inadequate healing of the subscapularis tendon can lead to postoperative pain, weakness, and instability.
Comment: We avoid lesser tuberosity osteotomy because it compromises the fixation of the humeral component in the metaphysis and obligates sacrifice of the long head tendon of the biceps.
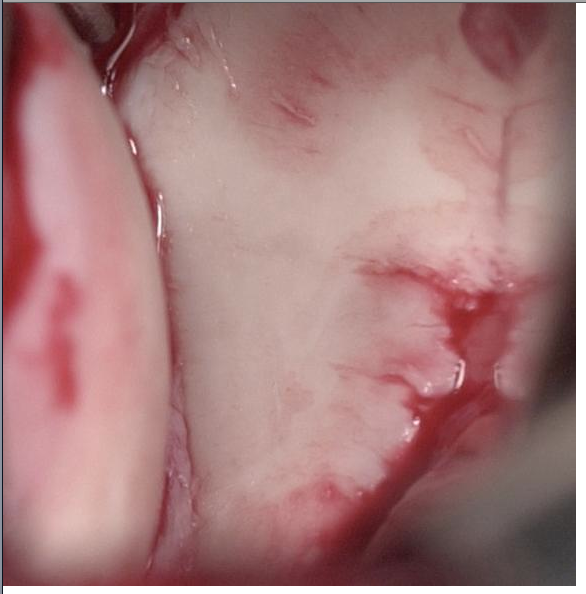
Our surgical approach involves a careful peel of the subscapularis tendon from the lesser tuberosity with attention to preserving the integrity of the biceps tendon and a 360 degree release of the capsule from the glenoid to resolve limitation of external rotation. By retaining the capsule on the deep surface of the tendon, the strength of the repair is enhanced.

At the conclusion of the case, drill holes are placed through good bone at the margin of the neck cut and six sutures of #2 non-absorbable suture are passed through these holes.


Rehabilitation after shoulder arthroplasty - cautions!
Our approach is to limit external rotation stretching to zero degrees (the hand shake position) and avoid internal rotation strengthening exercises for at least 3 months after surgery. We also caution patients about the risk of events that may suddenly externally rotate the shoulder such as a fall or a sudden pull on the arm from a leashed dog.

Other elated posts are listed below:
Subscapularis failure after arthroplasty - evaluation and management
The biomechanics of subscapularis repair - all sutures are not equal!
Subscapularis in shoulder arthroplasty
Shoulder joint replacement arthroplasty - spare the subscapularis, spoil the arthroplasty?
How well does the subscapularis work after total shoulder arthroplasty? ?Hazards of inter scalene block?
Failure of lesser tuberosity osteotomy in total shoulder joint replacement - a cautionary tale
Subscapularis failure after arthroplasty - evaluation and management
The biomechanics of subscapularis repair - all sutures are not equal!
Subscapularis in shoulder arthroplasty
Subscapularis and shoulder arthroplasty
The subscapularis - does it ever recover after shoulder arthropllasty - peel vs LTO?
The subscapularis - does it ever recover after shoulder arthropllasty - peel vs LTO?
===
To see the topics covered in this Blog, click here
Use the "Search" box to the right to find other topics of interest to you.
You may be interested in some of our most visited web pages including:shoulder arthritis, total shoulder, ream and run, reverse total shoulder, CTA arthroplasty, and rotator cuff surgery as well as the 'ream and run essentials'























{kind=link}
{kind=link}