
These authors described the characteristics, etiologies,and outcomes of 14 early (<3 months post op) and 5 late (>3 months post op) dislocations requiring operative revision. Their institutional rate of revision for instability after a reverse total shoulder was 2.7%.
63% of patients in both groups were men, were aged over 70 years (74±9 years), and 63% had a history of prior shoulder surgery.
68% had inadequate soft-tissue tensioning (10% due to partial axillary nerve injuries). The remaining patients had asymmetric liner wear, mechanical liner failure, or impinging heterotopic ossification. Asymmetric liner wear was present in 60% of late dislocations. Recurrent instability after revision occurred in 29% of early and 40% of late dislocators. Of the late dislocations, 80% had heterotopic ossification or asymmetric polyethylene wear.
Comment: Dislocation of a reverse total shoulder is not uncommon.











In fact, according to the Australian Joint registry, 1 in 20 reverse total shoulders require revision

and instability is the most common reason for revision.

In seeking to minimize the risk of post reverse total shoulder instability, we believe the following are helpful
(1) preoperative counseling about the need to keep the arm in mid-range positions for the first months after arthroplasty, especially if the reverse is being done for a failed prior arthroplasty or fracture fixation or if the patient is obese
(2) careful preoperative evaluation of deltoid function
(3) checking the tension of the reconstruction by applying traction to the arm and assuring there is no more than a millimeter or so of distraction of the humeral cup from the glenosphere
(4) examining the shoulder carefully with the trial components in place for unwanted contact between the humeral cup and the scapula in adduction, abduction, flexion, internal rotation and external rotation
(5) since many reverse total dislocations are anterior-superior, check the stability of the shoulder with the arm in adduction, internal rotation and extension (the 'waiter's tip' position)

Here's more on reverse total shoulder instability:
Treatment and Outcomes of Reverse Shoulder Arthroplasty Dislocations
These authors reviewed their experience with nonoperative and operative management of dislocated primary and revision reverse total shoulders (RSAs).
They reported that between 2006 and 2013, dislocation occurred in 12/1081 primary RSAs (1.1%) and 15/342 revision RSAs (4.4%).
Seventeen (69%) shoulders dislocated within 3 months of surgery.
After dislocation of a primary RSA, closed reduction was successful in 3 of 5 cases, while revision surgery was successful in 7 of 8 cases.
After dislocation of a revision RSA, closed reduction was successful in 1 of 5 cases, while revision surgery was successful in 7 of 11 cases.
Overall, 9 shoulders (33%) had persistent instability at the final follow-up: 2/12 (17%) primaries versus 7/15 (47%) revisions. Preoperative prosthetic instability was the main risk factor for chronic instability in the revision cohort . Worse functional outcomes were associated with the dislocation of a revision RSA and with female sex.
The case presented is instructional (see figures below the text):
An 80-year-old female who underwent primary RSA for rotator cuff arthropathy that sustained an anterior dislocation (a) of the prosthesis 1 year after surgery. The patient was initially managed with closed reduction but had continued instability events. She was then treated with upsizing of the polyethylene component during a modular exchange. (b) An intraoperative photograph of the polyethylene insert showing damage to the anterior lip from chronic instability events. Her shoulder remains stable at 2 years after revision (c).

Comment: A common cause of instability is unwanted contact between the humeral cup and th ebone of the scapula, as is suggested by figure (b) above. An alternate explanation for the polyethylene damage, as the authors suggest, is the trauma to the polyethylene that occurs with dislocation and reduction. Progressive damage to the rim of the humeral cup facilitates subsequent dislocations.
The take away lessons include:
(1) Before closing a reverse total shoulder procedure, examine the shoulder for unwanted contact, excessive laxity and for instability in all positions of the shoulder and resolve these issues before closure.
(2) In performing a reverse total shoulder for failed prior arthroplasty, recognize that instability is a major cause of complications - in these cases six weeks of postoperative immobilization may be helpful.
(3) Before and after surgery plan to minimize risk of falls, extreme positions, and unwanted loading.
More on this challenging problem can be found in this recent paper and below.
Dislocation following reverse total shoulder arthroplasty
These authors reviewed 22 patients having operative revision of a reverse total shoulder ( RTSA ) because of instability.
These authors reviewed 22 patients having operative revision of a reverse total shoulder ( RTSA ) because of instability.
Follow-up was obtained on 19 patients at 4.9 ± 2.5 years.
14 had early and 5 had late dislocations.
Most patients were men, were aged over 70 years, and had a history of prior shoulder surgery.
The authors believed that 13 had inadequate soft-tissue tensioning (2 due to partial axillary nerve injuries). The remaining patients had asymmetric liner wear, mechanical liner failure, or impinging heterotopic ossification.
Of the five late dislocations, 3 had asymmetric liner wear and 4 had evidence of unwanted contact between the humeral cup and the scapula.
Recurrent instability after revision was present in 4 of the 14 early and 2 of the 5 late dislocators.
Comment: While reverse total shoulder arthroplasty is often performed for glenohumeral instability, post-reverse total shoulder dislocation is one of the most important complications of this procedure. One of the interesting concepts is the role of unwanted contact between the medial humeral component and the lateral scapula as discussed here:
Impact of scapular notching on clinical outcomes after reverse total shoulder arthroplasty: an analysis of 476 shoulders
This is a welcome study, because scapular notching after a reverse total shoulder has often been written of has having 'no clinical consequence'.
The concern is not so much about the loss of bone at the scapular neck






Our technique reverse total shoulder arthroplasty is shown here: Reverse total shoulder technique









These authors retrospectively reviewed 448 patients who underwent a Grammont-type reverse total shoulder (461 shoulders) performed for rotator cuff tear arthropathy or osteoarthritis with cuff deficiency with a mean followup of 51 months (range, 24-206 months). They found notching of the scapula in 68% of the cases; it was present in 48% at one year after surgery.
These authors reviewed 476 shoulders at a minimum of 2 years after reverse total shoulder arthroplasty.

Scapular notching was observed in 10.1% (48 of 476) of rTSAs and was associated with a longer clinical follow-up, lower body weight, lower body mass index, and when the operative side was the non-dominant extremity.

Scapular notching was observed in 10.1% (48 of 476) of rTSAs and was associated with a longer clinical follow-up, lower body weight, lower body mass index, and when the operative side was the non-dominant extremity.
Patients with scapular notching had significantly lower postoperative scores on the Shoulder Pain and Disability Index, Constant, Simple Shoulder Test, and University of California, Los Angeles, Shoulder Rating Scale compared with patients without scapular notching.
Patients with scapular notching also had significantly lower active abduction and significantly less strength
Patients with scapular notching had a significantly higher complication rate.


This is a welcome study, because scapular notching after a reverse total shoulder has often been written of has having 'no clinical consequence'.
The concern is not so much about the loss of bone at the scapular neck

but rather the concern is what's causing the bone erosion.

In most cases, scapular notching is caused by unwanted contact between the polyethylene of the humeral cup and the bone of the scapula. While the effect on the scapular bone is evident on radiographs, the effect on the humeral polyethylene is only seen at the time of revision surgery.


Particles of polyethylene wear are known to cause inflammation, pain, stiffness and loosening.
A number of strategies can be used to avoid unwanted contract between the humeral polyethylene cup and the scapula. One is to use a glenoid component with lateral offset as shown on the right below.

Our technique reverse total shoulder arthroplasty is shown here: Reverse total shoulder technique
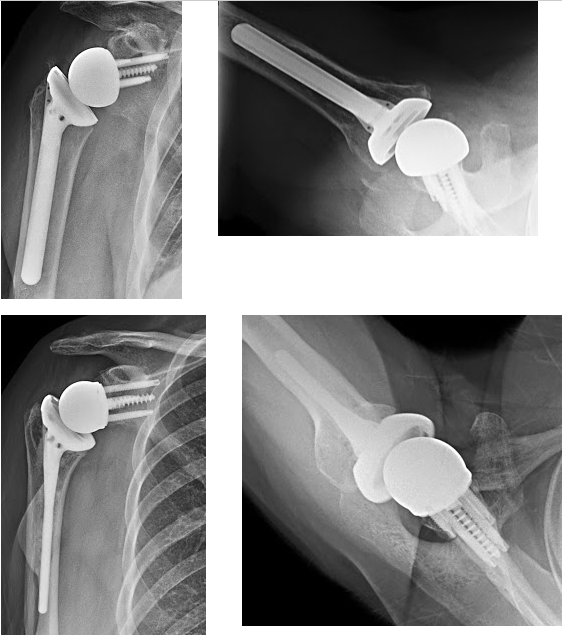
Here is the x-ray of a lady with a failed prosthesis for fracture. Note the superior displacement of the humeral head, the long cemented stem and the poor quality of the glenoid bone.

Her surgeon converted her to a reverse total shoulder with bone graft around the humeral component and a Grammont-style prosthesis

At two years after surgery, she had increasing shoulder pain and these films showing bone loss at the inferior aspect of her glenoid along with some evidence of contact between the lower screw and the humeral component.

Her most recent films show progressive loss of the bone supporting the glenoid component.

While this patient has yet to undergo a revision, we suspect that her humeral component may look like this.
This is a good time to review the article:
Anytime we have unintended contact between high density polyethylene and bone, it is a problem. Scapular notching is a radiographic finding, but the real concerns are about (1) the damage to the poly of the humeral cup, (2) loss of the bone of the scapula that supports the glenoid component, and (3) the potential for instability resulting from leverage of one against the other. See this previous post which discusses this phenomenon in some detail.
In the Grammont-type reverse total shoulder, contact of the adducted humeral component against the scapula is not uncommon as shown in these figures from a manufacturer's website (arrow inserted by us to show point of contact when the arm is brought to the side).

These authors retrospectively reviewed 448 patients who underwent a Grammont-type reverse total shoulder (461 shoulders) performed for rotator cuff tear arthropathy or osteoarthritis with cuff deficiency with a mean followup of 51 months (range, 24-206 months). They found notching of the scapula in 68% of the cases; it was present in 48% at one year after surgery.
Notching was more common in active patients, in patients with cuff tear arthropathy, and in patients with greater degrees of superior displacement of the humeral head before surgery. Strength and range of motion were compromised in patients with notching.
Importantly, 36% of shoulders with notching had humeral radiolucent lines (in contrast to 17% in those without notching), suggesting the possibility that polyethylene particles from the humeral cup causing bone resorption. Similarly glenoid loosening was three times more common in the presence of notching.
The authors point out that standardized plain x-rays are necessary for the evaluation of notching, noting that sometimes notching is better seen on the axillary view.
Scapular notching is important and can be expected to adversely affect the long term durability and function of the reverse. It is best avoided by (1) use of a glenoid component design that offsets the center of rotation from the scapula, (2) proper positioning of the glenoid component at the inferior aspect of the glenoid, (3) avoiding superior tilt of the glenoid component, and carefully checking for contact between the humeral component and scapula at surgery when the arm is adducted and rotated (see below).

To see a YouTube of our technique for a reverse total shoulder arthroplasty, click on this link.
=====
How you can support research in shoulder surgery Click on this link.
To see our new series of youtube videos on important shoulder surgeries and how they are done, click here.
Use the "Search" box to the right to find other topics of interest to you.
You may be interested in some of our most visited web pages arthritis, total shoulder, ream and run, reverse total shoulder, CTA arthroplasty, and rotator cuff surgery as well as the 'ream and run essentials'
To see our new series of youtube videos on important shoulder surgeries and how they are done, click here.
Use the "Search" box to the right to find other topics of interest to you.
You may be interested in some of our most visited web pages arthritis, total shoulder, ream and run, reverse total shoulder, CTA arthroplasty, and rotator cuff surgery as well as the 'ream and run essentials'