
After their review of the literature and their experience, these authors of this article thoughtfully conclude: " The humeral component is responsible for a small number of complications and revision surgeries in patients who undergo TSA. Therefore, long-term studies are necessary to determine if the results of shoulder arthroplasty with newer humeral components can match those of shoulder arthroplasty with older humeral components and warrant the additional cost associated with their use."

These authors point out that some common pathologies, such as rheumatoid arthritis, osteoporosis, and large subchondral cysts are relative contraindications to a stemless implant because they may preclude its stable anchorage.
Comment: As pointed out recently in "Complications of Shoulder Arthroplasty" (see this link), humeral component loosening with a conventional stem accounts for a very small percentage of total shoulder complications.

While it is stated that stemless humeral components are beneficial because they allow for anatomic reconstruction independent of the shaft axis and the posterior offset of the proximal humerus, it is not clear that these issues have been clinical problems in the hundreds of thousands of arthroplasties performed with conventional stems.
The stemless prosthesis is said to be 'canal sparing', yet the canal of the humerus is a space filled with fatty tissue that has replaced the marrow.
The stemless prothesis is said to reduce the risk of intraoperative humeral shaft fracture, yet in one of the references, 5 of 61 patients with osteoarthritis undergoing stemless shoulder arthroplasty had an intraoperative lateral humeral cortical fracture. In another study, the overall complication rate was 12.8%, and the overall revision surgery rate was 9%, percentages substantially higher than those for shoulder arthroplasties with conventional stemmed humeral fixation.
Other proposed advantages of the stemless humeral implant are reduction of the risk of traumatic periprosthetic humeral shaft fracture as a result of a stress riser at the distal tip of the implant, decrease in the risk of stress shielding, and reduction of the risk of stem revision. However, these risks area also reduced by the use of a thin, smooth, impaction grafted stem as shown below.
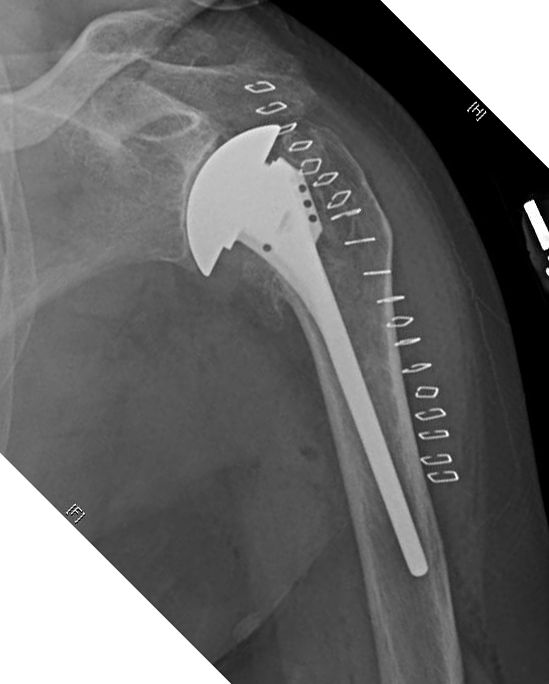
Clinical experience has indicated that stemless prostheses have their own learning curve and set of potential problems of fixation and positioning as shown in the films below.


We find in the great majority of cases, the proposed advantages of "canal sparing" prostheses can be achieved with impaction grafting of a thin smooth stem: preservation of humeral bone stock for potential revisions, performance of anatomic reconstruction regardless of posterior offset in anatomic arthroplasty, facilitating arthroplasty in cases of humeral deformity, prevention of malpositioning, and avoiding periprosthetic fractures. Furthermore, the impaction grafted smooth stem can be used in almost all anatomic arthroplasties, without the relative contraindications for a stemless humeral component: cysts, inflammatory arthritis, and osteoporosis.
The variations of intramedullary anatomy are recognized

and managed by impacting humeral autograft into the canal, 'reinvesting' the patients own bone in strengthening the humeral shaft.

This approach enables precise positioning of a humeral component with a smaller stem, secure safe fixation, and ease of prosthesis exchange should revision become necessary. Note the absence of cortical contact with the tip of the prosthesis and the absence of stress shielding.


It also allows the use of an anteriorly eccentric humeral head to manage posterior instability, a modification not possible with stemless implant.


It is apparent that management of a post traumatic arthritic shoulder can be complicated if the humerus is malunited in varus.

because normal positioning of the humeral component would conflict with the cuff attachment to the tuberosity.

In these cases it is possible to use impaction grafting to fix a small stemmed humeral prosthesis in an amount of varus that matches the deformity, so that the humeral head is positioned in the center of the glenoid. In the case below, the fixation of the humeral component was robust - more than what we could have achieved with a stemless prosthesis.
Here's another humeral deformity managed with a thin stem and impaction grafting.


Thus it seems that at present, achieving competence and confidence with a smooth, thin, impaction-grafted stem provides the most universal approach to humeral arthroplasty - short stemmed or stemless implants have yet to show clinical superiority to this technique in the great majority of patients.
===
The reader may also be interested in these posts:
Information about shoulder exercises can be found at this link.
Use the "Search" box to the right to find other topics of interest to you.
You may be interested in some of our most visited web pages including:shoulder arthritis, total shoulder, ream and run, reverse total shoulder, CTA arthroplasty, and rotator cuff surgery as well as the 'ream and run essentials'See from which cities our patients come.