
These authors sought to determine the results, complications, and failure rate among 43 patients with a self-reported metal allergy undergoing shoulder arthroplasty. Overall 1.6% of all their shoulder arthroplasty patients reported metal allergies.
Allergies reported included nickel (37), cobalt chrome (4), copper (2), zinc (1), titanium (1), gold (1), and nonspecific metal allergy (8); 8 patients reported multiple metal allergies. All components implanted in patients with nickel allergies contained nickel. At most recent follow-up, pain was rated as none or mild in 88% of shoulders. Active elevation improved from 80 to 141and external rotation from 24 to 52. Two revisions were performed for glenoid loosening (3.8%); both were revision cases with substantial glenoid bone loss. One patient with mild pain had a radiographically loose glenoid component 12 years after anatomic shoulder arthroplasty.
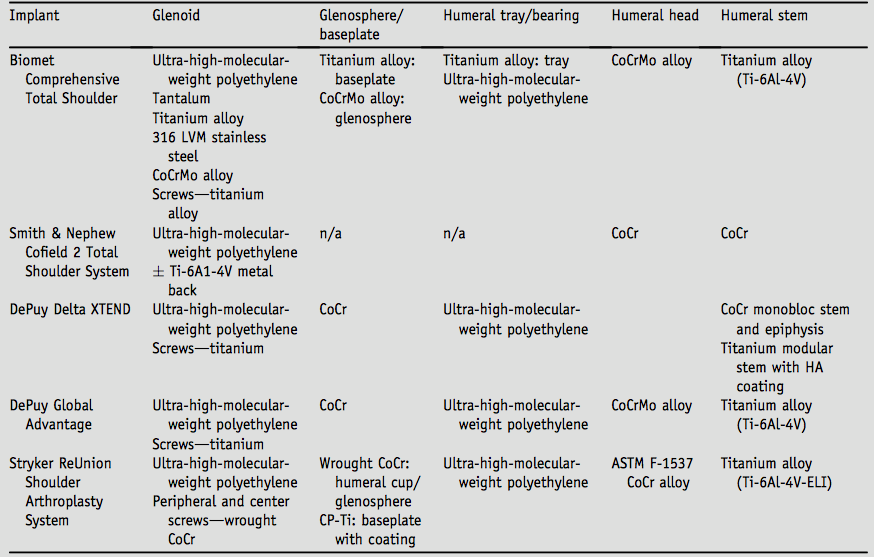
Their chart provides a useful insight into the metal content of some current arthroplasty systems
The authors point out that while skin patch testing is the gold standard for determining metal hypersensitivity and recommended for patients with a history of dermatitis prior to metallic implantation, prior studies have also shown no correlation between positive skin patch test results and outcomes in orthopedic arthroplasty surgery and that there is poor correlation between self-reported allergy and skin patch results, with only 30% of patients with a self-reported nickel allergy having a positive skin patch test.
All of the patients in this series had improvements in range of motion and pain relief after shoulder arthroplasty. This is in agreement with other arthroplasty studies, which have shown no increased complications in patients with metal allergies who have undergone hip or knee replacements with standard implants. In hip and knee patients with patch test–positive metal allergies, surgeons have reported no complications or symptoms associated with use of standard metallic implants.
Comment: Stimulated by this article, we reviewed over 100 articles discussing metal allergy and its relationship to total joint arthroplasty outcome. From this review we concluded:
(1) There is an inconsistent relationship between self reported metal allergies and skin tests.
(2) Patients with self-reported metal allergies and/or positive skin tests do not have worse outcomes when standard implants are used.
(3 There are no specific clinical tests for metal allergy that have demonstrated utility in the evaluation of patients with failed arthroplasty.
(4) No distinctive surgical findings of metal allergy have been identified at revision surgery that distinguish this proposed etiology of failure from others.
(5) While some patients with suspected metal allergy have good results after revision with a hypoallergenic set of implants, these results have not been demonstrated to be superior to those of revision with standard implants.
These authors point out that the utilization of lymphocyte transformation testing (LTT) has increased for diagnosing metal sensitivity associated with knee arthroplasty, but its validity for the diagnosis of TKA failure due to an immune reaction has not been established. They sought to characterize the relationship of a positive LTT result to histopathologic findings and clinical and functional outcomes in 27 well-fixed, aseptic, primary TKA cases in which the patient had persistent pain and/or stiffness and underwent revision due to a suspected metal allergy to nickel, as determined on the basis of positive LTT. Periprosthetic tissue samples obtained at the time of revision surgery were scored using the aseptic lymphocyte-dominated vasculitis-associated lesion (ALVAL) scoring system.
Eight patients were categorized as mildly reactive; 8 patients, moderately reactive; and 11 patients, highly reactive to nickel by LTT. The predominant findings on routine histopathologic analysis were fibrosis and varying degrees of lymphocytic infiltration in 17 (63%) of the 27 cases. The average ALVAL score of the cohort was 3.1 +/- 1.9, of a maximum score of 10. Average Knee Society Score (KSS) values improved post-revision, as did range of motion (all p < 0.01).
Neither LTT stimulation index as a continuous variable nor as a categorical variable (mildly reactive, moderately reactive, highly reactive) was correlated with ALVAL score, pre-revision function (as assessed by KSS-clinical, KSS-functional, and range of motion), or change in function at the most recent follow-up (0.015 < r < 0.30, 0.13 < p < 0.95). In addition, the ALVAL score did not correlate significantly with either pre-revision or post-revision KSS or range of motion (0.061 < r < 0.365, 0.09 < p < 0.88).
The authors concluded that LTT results alone were insufficient for the diagnosis of TKA failure due to an immune reaction. A positive LTT may not indicate that an immune reaction is the cause of pain and stiffness post-TKA.
===
We have a new set of shoulder youtubes about the shoulder, check them out at this link.
Be sure to visit "Ream and Run - the state of the art" regarding this radically conservative approach to shoulder arthritis at this link and this link
Use the "Search" box to the right to find other topics of interest to you.
You may be interested in some of our most visited web pages arthritis, total shoulder, ream and run, reverse total shoulder, CTA arthroplasty, and rotator cuff surgery as well as the 'ream and run essentials'