
The balloon received Food and Drug Administration (FDA) clearance in the USA in July, 2021, with approximately 29,000 devices having been implanted outside the USA before this.

The question is, in patients with symptomatic, irreparable rotator cuff tears, does adding a subacromial balloon spacer to debridement alone improve shoulder pain and function above what is achieved with debridement alone?
While small published case series have suggested encouraging clinical results, others have reported poor results or cases of inflammation and pain. For this reason, the authors of Subacromial balloon spacer for irreparable rotator cuff tears of the shoulder (START:REACTS): a group-sequential, double-blind, multicentre randomised controlled trial conducted a novel, efficient, adaptive clinical trial to assess the clinical effectiveness of a subacromial spacer balloon for people with symptomatic irreparable tears of the rotator cuff. This article was summarized in In Symptomatic Irreparable Rotator Cuff Tears, Adding a Subacromial Balloon Spacer to Debridement Resulted in Worse Shoulder Pain and Function at 12 Months.
The study was conducted by surgeons in 24 hospitals in the United Kingdom and included 117 patients (mean age, 67 years; 57% men) who had irreparable rotator cuff tears with disabling symptoms (pain and loss of function) and unsuccessful nonoperative management, and in whom surgery was warranted. Patients with reparable cuff tears, arthritis, pseudoparalysis, and subscapularis deficiency were excluded.
Eligibility was confirmed intraoperatively before randomly assigning (1:1) participants to a treatment group using a remote computer system. Using concealed allocation, patients were randomized to balloon spacer plus debridement (n = 56) or debridement alone (n = 61). Patients in the balloon spacer group received the Stryker InSpace balloon inserted by subspecialty-trained shoulder surgeons after arthroscopic debridement of the subacromial space and biceps tenotomy. Participants and assessors were masked to group assignment. Masking was achieved by using identical 1.5-cm lateral portal incisions for both procedures, blinding the operation note, and a consistent rehabilitation program offered regardless of group allocation.
The study was designed to have 90% power providing a robust answer to the clinical question.
The primary outcome was shoulder-related pain and function as measured by the Oxford Shoulder Score at 12 months. Secondary outcomes included the Western Ontario Rotator Cuff Index, EuroQol-5 Dimensions-5 Levels (EQ-5D-5L), and adverse events at 12 months. 97% of patients completed follow-up for the primary outcome. The primary outcome was the Oxford Shoulder Score at 12 months.
Pre-trial simulations using data from early and late timepoints informed stopping boundaries for two interim analyses. The study was designed to be terminated either for convincing evidence of a lack of benefit (futility) or for strong clinical benefit (efficacy). This exposes fewer people to risk of harm in the trial itself, as well as preventing harm or high costs for people having the treatment in the wider community. Having both futility and efficacy stopping rules allow a study to report early if an intervention is ineffective. Recruitment to this study was stopped when the predefined boundary for futility was crossed.
As seen in the figure and table below, in patients with symptomatic irreparable rotator cuff tears, adding the InSpace balloon to debridement only resulted in worse shoulder pain and function. The mean Oxford Shoulder Score at 12 months was 34·3 (SD 11·1) in the debridement only group and 30·3 (10·9) in the debridement with device group (mean difference adjusted for adaptive design –4·2 [95% CI –8·2 to –0·26];p=0·037) favoring debridement alone.



The adverse events for the two groups are shown below.

The authors concluded that for patients with symptomatic irreparable rotator cuff tears, adding a subacromial balloon spacer to debridement resulted in worse shoulder pain and function at 12 months.
Another recent study, InSpace Implant Compared with Partial Repair for the Treatment of Full-Thickness Massive Rotator Cuff Tears A Multicenter, Single-Blinded, Randomized Controlled Trial concluded that the outcomes of the InSpace implant were not inferior to those of partial repair for the treatment of patients with irreparable, posterosuperior, massive rotator cuff tears and an intact subscapularis.


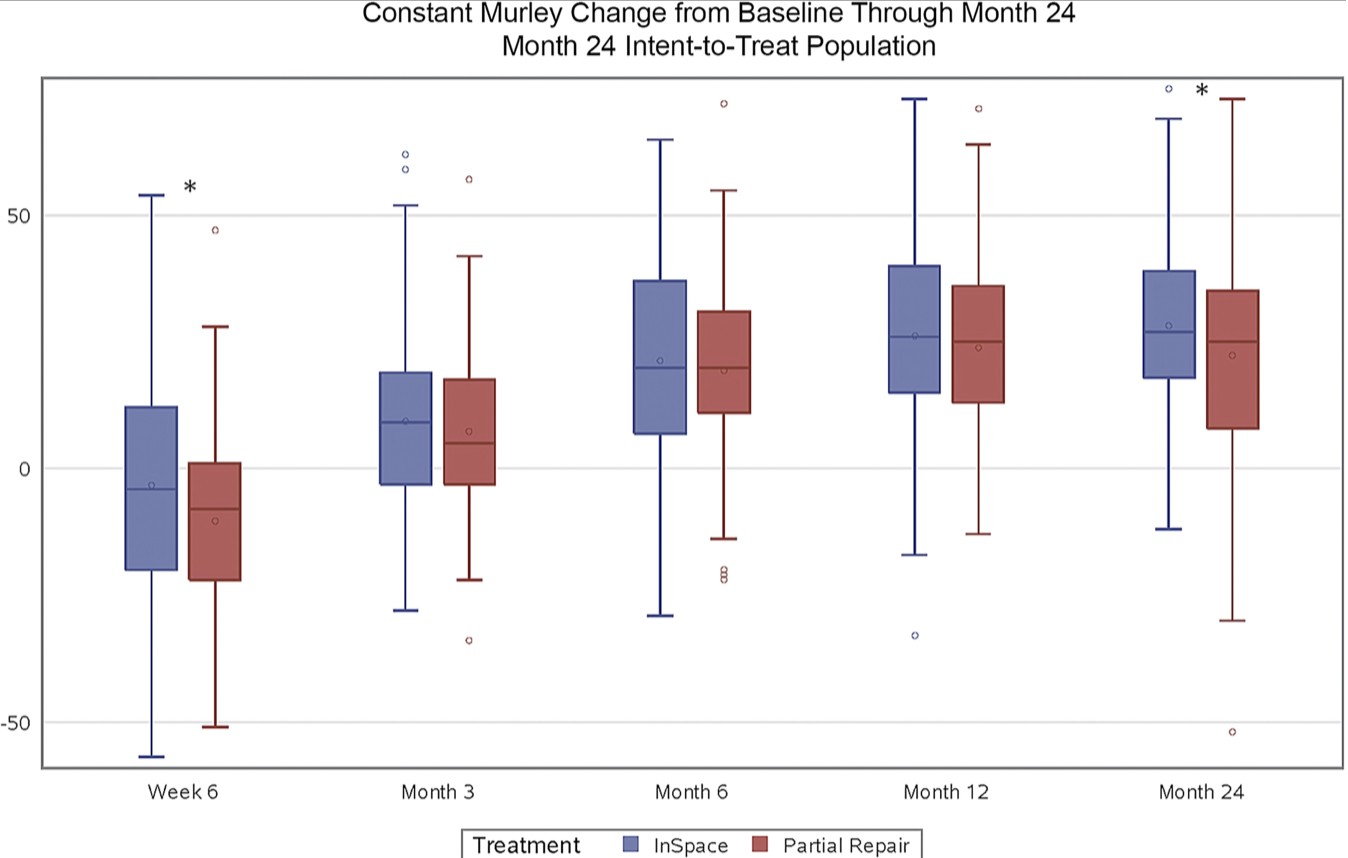
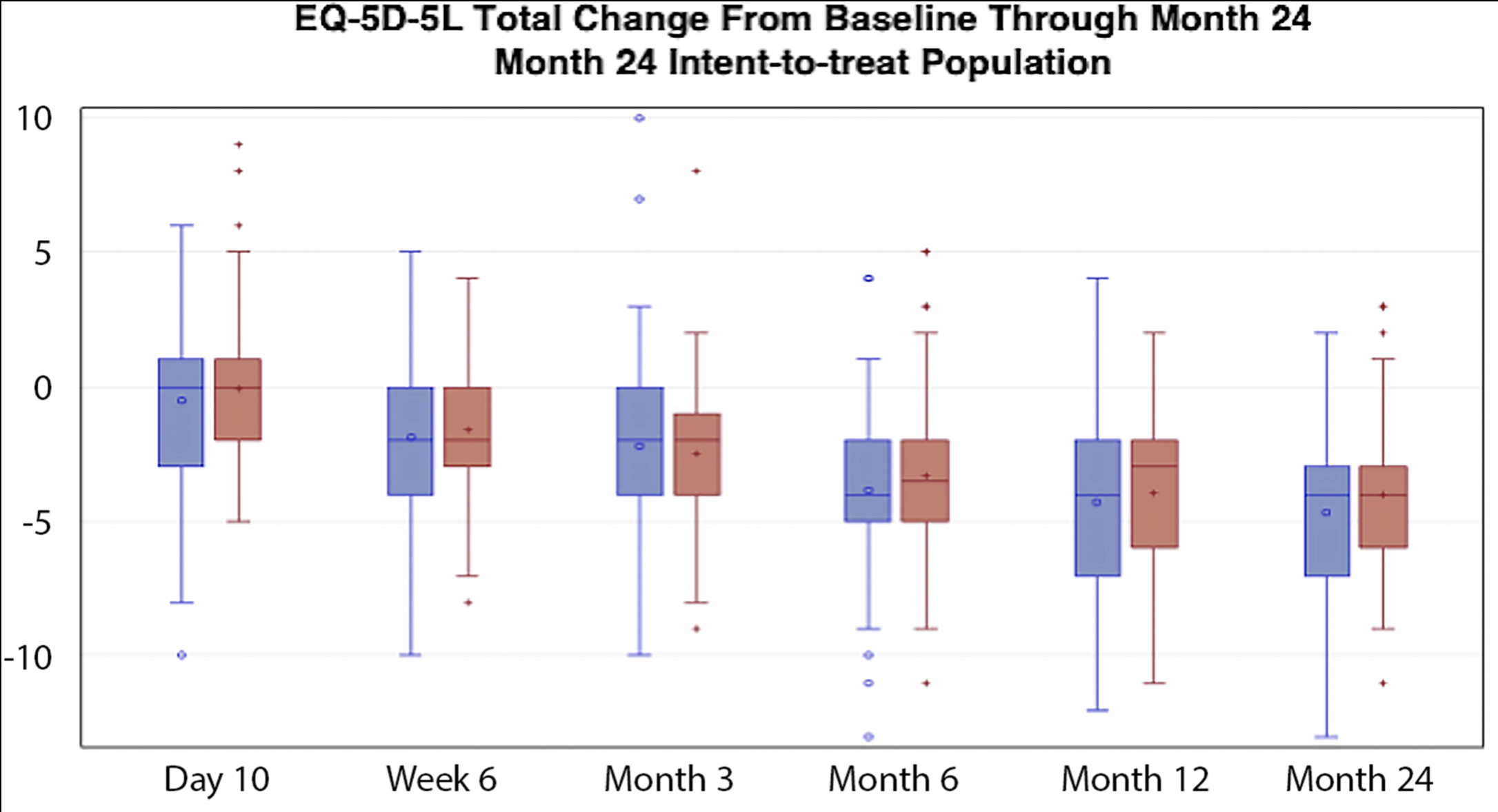

The authors of this second study described its limitations, including the fact that the evaluators of the physical examination were not blinded with respect to treatment groups.
Comment: These studies do not provide evidence of increased effectiveness of the InSpace balloon in comparison to debridement or partial cuff repair.
You can support cutting edge shoulder research that is leading to better care for patients with shoulder problems, click on this link.
To add this blog to your reading list in Google Chrome, click on the reading list icon

Follow on twitter: https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link).
Shoulder rehabilitation exercises (see this link).