At a recent journal club (thanks, Ben, for organizing), we discussed antibiotic prophylaxis for periprosthetic infections (PJI). It is known that multiple different organisms can cause PJI, but - especially in young healthy males - Cutibacterium is most commonly the culprit. We can provide a bit of an update on some of the key questions
(1) What is the best IV prophylactic antibiotic?
Cephalosporins seem superior as reported in Antibiotic Prophylaxis with Cefazolin Is Associated with Lower Shoulder Periprosthetic Joint Infection Rates Than Non-Cefazolin Alternatives. Among 7,713 shoulder arthroplasties 101were classified as having PJIs. Cutibacterium was identified in 44%, Staph aureus in 19%, Coagulase-negative staph in 12%, and Strep in 5%.
Cefazolin had been administered in 6,879 procedures (89.2%) and non-cefazolin antibiotics (vancomycin, clindamycin, and alternative regimens were administered in 834 procedures (10.8%).
PJI-free survivorship was greater in shoulder arthroplasties in which cefazolin was administered compared with those in which non-cefazolin antibiotics were administered. Cefazolin administration, compared with non-cefazolin administration, was associated with a 69% reduction in all-cause PJI risk and a 78% reduction in C. acnes PJI risk.
A higher risk of PJI for both groups was observed with vancomycin; the hazard ratio [HR] was 2.32 for all-cause PJI and 2.94 for Cutibacterium PJI. A higher risk of PJI was also observed for both groups for clindamycin; the HR was 5.07 for all-cause PJI and 8.01 for Cutibacterium PJI. The latter may be due to the pervasive use of clindamycin as a treatment for acne - a practice that may select out clindamycin resistant Cutibacterium.
It is of interest that half of the periprosthetic infections were identified more than two years after the index arthroplasty - this complicates the analysis of antibiotic efficacy in studies with only a couple of years of followup.
(2) Is Clindamycin a good alternative for patients reporting penicillin allergy?
This question was addressed in Perioperative Clindamycin Use in Penicillin Allergic Patients Is Associated With a Higher Risk of Infection After Shoulder Arthroplasty. This study reviewed seven thousand one hundred forty primary shoulder arthroplasties comparing deep surgical site infection risk in 444 patients who received perioperative vancomycin alone or 508 receiving clindamycin alone because of penicillin allergy to 6188 patients who received cefazolin alone without penicillin allergy.
Seventy deep infections were observed; most common organism was Cutibacterium acnes (39.4%).
Compared with patients treated with cefazolin, infection risk was not different for those treated with
vancomycin, but a higher risk of infection was identified for those treated with clindamycin alone. Thus in contrast to the first study above, these authors concluded that vancomycin is preferred over clindamycin for patients with penicillin allergy. Other studies have demonstrated that patients with multiple allergies have a poorer average prognosis after arthroplasty; one might also wonder whether patients with allergies to penicillin are more susceptible to infection independent of which antibiotic is used.
(3) How can we tell if patient-reported allergy should change the antibiotic choice?
This question was addressed in A Simple Algorithmic Approach Allows the Safe Use of Cephalosporin in “Penicillin-Allergic” Patients without the Need for Allergy Testing. These authors point out that patients who report a penicillin allergy are often given second-line antibiotic prophylaxis during total joint arthroplasty. As seen from the article above, the use of non-cephalosporin antibiotics exposes the patient to an increased risk of PJI. These authors assessed the effectiveness of a simple penicillin allergy screening program to guide the choice of antibiotic prophylaxis.
Basically patients were grouped into three groups
"intolerance",
"low risk allergy"
and "high risk allergy"
The "intolerance" and " low-risk"patients received cefazolin, and the high-risk cohort received non-cefazolin antibiotics.
The protocol group (n = 2,078) was propensity score matched 1:1 with a control group that included patients who underwent TJA in the same institution prior to implementation of the protocol, the "control" group.
A total of 357 patients (17.2%) reported a penicillin allergy in the protocol group compared with 310 patients (14.9%) with a recorded allergy in the control group (p = 0.052).
The number of patients who received non-cephalosporin antibiotics was significantly lower in the protocol group (5.7% compared with 15.2% in the control group; p < 0.001),whereas there was no difference in the rate of total allergic reactions.
Of the 239 low-risk patients (66.9%) in the protocol group, only 3 (1.3%) experienced a mild cutaneous reaction following cefazolin administration.
There were no differences in the rates of superficial wound, deep periprosthetic, or Clostridioides difficile infections between the protocol and control groups.
(4) Is there evidence that topical Vancomycin is effective against Cutibacterium?
Vancomycin is effective in preventing Cutibacterium acnes growth in a mimetic shoulder arthroplasty
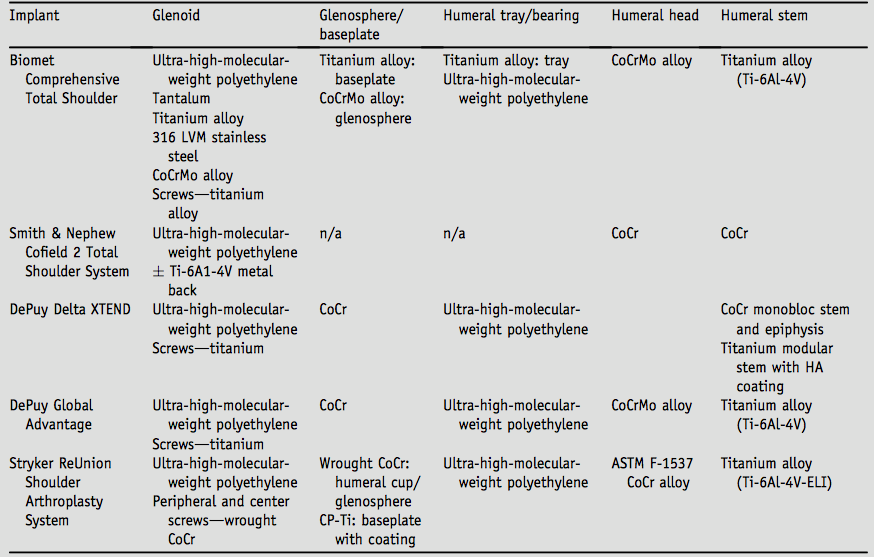
Cutibacterium loves to form biofilms on titanium alloy - one of the most common materials used in shoulder arthroplasty. We recognize that in spite of all available prophylactic measures (skin prep, IV antibiotics), arthroplasty wounds are likely to be inoculated with Cutibacterium. This is especially an issue with patients at high risk (young, healthy males, with high skin surface loads of Cutibacterium and with high serum testosterone levels) as well as those patients truly allergic to cephalosporin antibiotics.
Topical vancomycin powder is a strategy for managing Cutibacterium inoculation at the time of shoulder arthroplasty. Its efficacy is difficult to test through clinical research.
These authors investigated the efficacy of vancomycin as prophylaxis for Cutibacterium growth in vitro using a mimetic shoulder arthroplasty.
Cutibacterium strains were applied to titanium alloy foil and embedded beneath multiple layers of collagen-impregnated cellulose scaffold strips containing human shoulder joint capsular fibroblasts, facilitating the development of an oxygen gradient with an anaerobic environment around the foil and inner layers. Agar plates inoculated with extracts from untreated constructs consistently resulted in the growth of large numbers of C acnes colonies
Ten milligrams of vancomycin powder was applied between the C acnes layer and the human cell–containing scaffold strips to model direct antibiotic application.
Intravenous vancomycin prophylaxis was modeled by adding vancomycin in media at 5 or 20 mg/mL. Treatments with vancomycin powder or vancomycin in media at 20-mg/mL dilution effectively prevented the recovery of any C acnes colonies. However, the lowest vancomycin dilution tested (5 mg/mL) was insufficient to prevent the recovery of C acnes colonies.
Vancomycin powder had no discernible short-term impact on shoulder capsule cell morphology, and the presence of these cells had no discernible impact on vancomycin degradation over time.
The authors concluded that topical vancomycin powder and high levels of vanancomycin in the media effectively prevented C acnes growth in a mimetic model of the shoulder arthroplasty environment.
In our practice we use topical vancomycin powder in the medullary canal and in the wounds of shoulder arthroplasties, noting that the topical application avoids the risks and inconvenience of systematic vancomycin.
You can support cutting edge shoulder research that is leading to better care for patients with shoulder problems, click on this link.
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link). How to x-ray the shoulder (see this link). The ream and run procedure (see this link). The total shoulder arthroplasty (see this link). The cuff tear arthropathy arthroplasty (see this link). The reverse total shoulder arthroplasty (see this link). The smooth and move procedure for irreparable rotator cuff tears (see this link). Shoulder rehabilitation exercises (see this link).