A 20 year old woman had an arthroscopic instability repair of her shoulder followed by the intra articullar infusion of local anesthetics through a pain pump. After surgery she had pain and stiffness of her shoulder. X-rays taken 10 months after surgery show joint space narrowing.

Seventeen years after her arthroscopic surgery at the age of 37 she presented to us with a very stiff shoulder. She had essentially no glenohumeral motion. Her x-rays at that time are shown below


Because of her physically active life style she wished to proceed with a ream and run procedure.
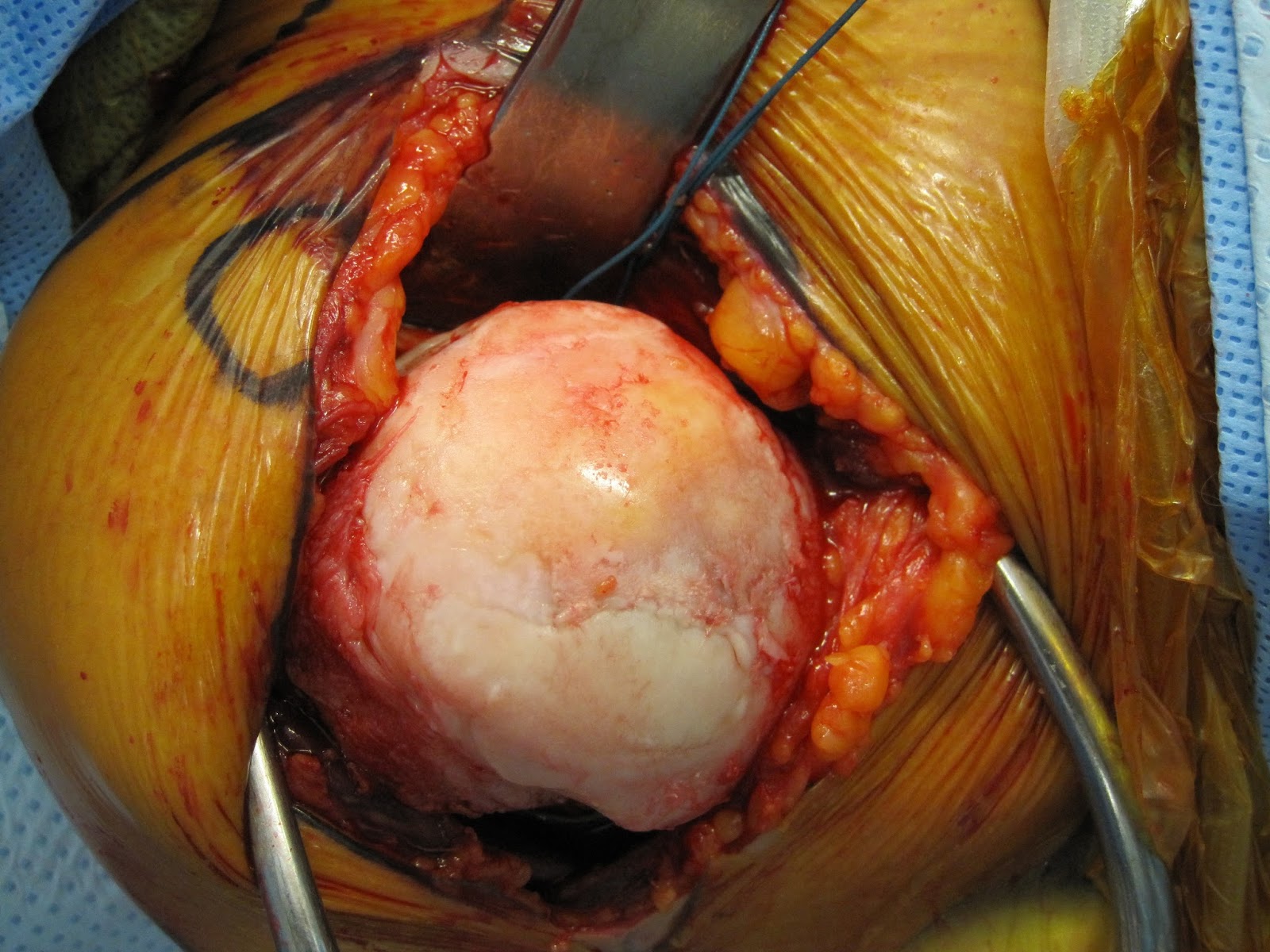
The appearance of her humeral head and glenoid at surgery are shown below






Published Evidence Demonstrating the Causation of Glenohumeral Chondrolysis by Postoperative Infusion of Local Anesthetic Via a Pain Pump
The joint surfaces of the shoulder (glenohumeral) joint are normally covered by smooth articular cartilage.

Glenohumeral chondrolysis is the irreversible destruction of previously normal articular cartilage, occurring most commonly after shoulder surgery in young individuals.

The reported incidence of this complication has risen rapidly since the early 2000s. As chondrolysis cannot be reversed, its occurrence can only be prevented by establishing and avoiding its causes.
The authors analyzed all published cases of glenohumeral chondrolysis, including the relevant published laboratory data, to consolidate the available evidence on the causation of this complication by the postoperative intra-articular infusion of local anesthetic via a pain pump.
The published evidence demonstrated a causal relationship between the infusion of local anesthetic and the development of glenohumeral chondrolysis.

The risk of this complication in shoulders receiving intra-articular infusions via a pain pump was significantly greater with higher doses of local anesthetic: twenty of forty-eight shoulders receiving high-flow infusions developed chondrolysis, whereas only two of twenty-five shoulders receiving low-flow infusions developed this complication (p = 0.0029). Eleven of twenty-two shoulders receiving 0.5% bupivacaine developed chondrolysis, whereas none of six shoulders receiving 0.25% bupivacaine developed this complication (p = 0.05). Of twenty-two shoulders infused with 0.5% bupivacaine, the eleven that developed chondrolysis had a mean pain pump delivery volume of 377 mL, whereas the eleven that did not develop chondrolysis had a mean volume of 187 mL (p = 0.003). Among shoulders in which an intra-articular pain pump was used, the risk of chondrolysis was significantly greater when suture anchors were placed in the glenoid for labral repair (p < 0.001). The effect seen with suture anchors may be due to the fact that they allow the intraarticular local anesthetic otherwise present only at the joint surface (green in the figure below)
 to gain access to the deeper tissue through the hole in the cartilage associated with the suture anchor.
to gain access to the deeper tissue through the hole in the cartilage associated with the suture anchor.
It was concluded from the published evidence indicates that the preponderance of cases of glenohumeral chondrolysis can be prevented by the avoidance of the intra-articular infusion of local anesthetic via a pain pump.
As we've emphasized before (see here), two plain x-rays are necessary and sufficient to make most diagnoses of shoulder arthritis.
Here is an anteroposterior (AP) and an axillary view typical of shoulders with chondrolysis from the intraarticular infusion of local anesthetics with a pain pump.
The upper view, the AP shows an atrophic joint without sclerosis or osteophytosis, and with osteopenia and articular surface cysts.

The standardized axillary view reveals much more of the pathology: central erosion of the glenoid and shows the loss of humeral head roundness as well as the articular surface cysts.

Chondrolysis and pain pumps 2
Chondrolysis and pain pumps 3
Chondrolysis and pain pumps 4
Toxicity of local anesthetics
Risk factors for chondrolysis
x-rays in chondrolysis
x-rays in chondrolysis 2
Case 1
Case 2
Case 3
Postarthroscopic Glenohumeral Chondrolysis PAGCL JAAOS
In other joints
Post arthroscopic glenohumeral chondrolysis ?review
Chondrolysis - ?review
To support our research to improve outcomes for patients with shoulder problems, click here.
To subscribe to this blog, enter your email in the box to your right that looks like the below

===
We have a new set of shoulder youtubes about the shoulder, check them out at this link.
Be sure to visit "Ream and Run - the state of the art" regarding this radically conservative approach to shoulder arthritis at this link and this link
Use the "Search" box to the right to find other topics of interest to you.