At followup, there were no statistical or clinically relevant differences in WOOS or patient-reported outcomes between the two groups.
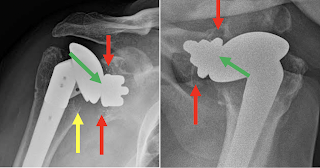
Metal debris was observed in 11 (23.9%) of the TM shoulders without apparent impact on clinical outcomes.

One TM patient experienced glenoid loosening in the setting of an infection.
One POLY patient had a minor intraoperative periprosthetic fracture of the glenoid which resolved non-operatively.
Otherwise there was no radiographic evidence of glenoid loosening in either group.
Comment: This randomized clinical trial showed a minimal rate of glenoid component failure at five years after anatomic total shoulder arthroplasty for both the uncemented trabecular metal-backed glenoid and the cemented non-ingrowth polyethylene glenoid in patients undergoing a total shoulder arthroplasty. They noted no differences in outcome between the two glenoid components.
The authors point out that the osseous integration seen with the TM glenoid has the negative consequence that occurs in the revision setting where prosthesis removal can be extremely challenging and lead to extensive bone loss.
You can support cutting edge shoulder research and education that are leading to better care for patients with shoulder problems, click on this link.
Follow on twitter: https://twitter.com/RickMatsen or https://twitter.com/shoulderarth
Follow on facebook: click on this link
Follow on facebook: https://www.facebook.com/frederick.matsen
Follow on LinkedIn: https://www.linkedin.com/in/rick-matsen-88b1a8133/
Here are some videos that are of shoulder interest
Shoulder arthritis - what you need to know (see this link).
How to x-ray the shoulder (see this link).
The ream and run procedure (see this link).
The total shoulder arthroplasty (see this link).
The cuff tear arthropathy arthroplasty (see this link).
The reverse total shoulder arthroplasty (see this link).
The smooth and move procedure for irreparable rotator cuff tears (see this link).
Shoulder rehabilitation exercises (see this link).